Arthritis
Richard A. Bernstein
Douglas M. Sammer
Marco Rizzo
Charles S. Day
Louis W. Catalano III
Brian D. Adams
Karim Barki
Seth D. Dodds
Kevin J. Malone
Steven L. Moran
Christina M. Ward
Inflammmatory Arthritis
I. Seropositive
Inflammatory arthropathies include the classic seropostive arthritic variants such as rheumatoid arthritis (RA), and those that are considered seronegative such as psoriatic arthritis (PsA) and ankylosing spondylitis. By far, the most common form of inflammatory arthritis is RA.
RA is an inflammatory disease affecting about 2.1 million people in the United States with its associated features of pain, swelling, stiffness, and loss of function in the joints. As an inflammatory process consisting of spontaneous proliferation of the synovial cells of joints and those lining tendon sheaths, the classic features include spontaneous, often symmetrical joint swelling and stiffness. This progresses to soft tissue disruption of the supporting structures of the affected joints, overgrowth of the synovial layer (pannus) over the articular cartilage, eventually destroying this as well. The similar, synovial proliferative, process can occur with tendons with associated tenosynovitis, adhesions, and eventual rupture. Both flexors and extensors can be involved.
There have been major advancements in the medical treatment of this condition, resulting in decreased need for operative treatment. Despite this, individuals with aggressive forms of the disease, nonresponsive to medical management, will continue to benefit from surgical intervention.
General conditions related to the upper extremity
Bone quality
Osteopenia
Periarticular osteolysis
Bone loss
Auto fusion
Soft tissue issues relevant to surgery
Contractures and deformity
Laxity
Tendon issues
Subluxation
Dislocation
Ruptures
Wrist
Deformities
Radial deviation of the carpus and metacarpals, volar subluxation of the carpus
Autolysis of carpal bones, with or without partial spontaneous arthrodesis
Ulnar head dorsal dislocation secondary to carpal supination and synovitis of the distal radioulnar joint (DRUJ)
Ruptures of the extensor tendons (caput ulnae syndrome)
Surgical management
Synovectomy alone rarely indicated
Limited arthrodesis: Radiolunate (Chamay)
Total wrist arthrodesis: The gold standard
Techniques of wrist fusion:
Pin/rod
Plate and screws
Expected results
High level of patient satisfaction
Reduction or elimination of pain in almost all patients
Functional impairment for fine motor tasks documented
Bilateral issues: Fuse both in slight extension, poor satisfaction with flexion (perineal care) in nondominant wrist
Arthroplasty: Evolving technology
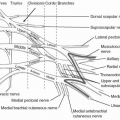
Caput ulnae syndrome
Ulnar head resection or arthroplasty and stabilization
Tendon repair or transfers (tendon fraying occurs frequently over a wide area and repair is often not possible)
Metacarpal phalangeal joints
Pathomechanics of deformities at the metacarpophalangeal (MCP) level: Joint destruction begins early in the disease, associated with three phases:
Initial proliferative phase
Pain, effusion
Synovial proliferation, angiogenesis
Destructive phase
Synovial pannus invades cartilage and soft tissue
Late phase (“Burnt Out”)
Less inflammation, replaced by fibrosis scarring and fixed deformities
Ulnar drift consists of both ulnar shift and ulnar deviation.
Normal MP joint is condylar, allows multiaxial movements, relies upon capsule and ligaments to provide stability.
Synovial proliferation and destruction result in laxity of the collateral ligaments.
Dorsal structures stretch.
Extensor hood weakened at the level of the sagittal bands, allowing ulnar subluxation of the tendons (i.e radial sagittal bands compromised).
Wrist radial posturing along with wrist ulnar translocation encourages the ulnar shift of the tendons secondary to the axial load direction that is altered by the wrist position.
Volar subluxation or dislocation occurs because of collateral ligament weakening and with the flexors overpowering the weakened extensors.
Dorsal extensor mechanism and capsule stretched and rendered less effective by dislocated position.
This imbalance at both levels, the joint and the extrinsic tendons results in the ulnar drift and volar subluxation of the digits at the MP level.
Loss of function
Dependent on the extent of the deformity
Function can be well preserved until late
Deformity
Aesthetic appearance
“Declaration of having a disease”
Current methods of surgical management
Synovectomy alone
i) Synovectomy
Alone is rarely indicated
May rarely be used for a joint, which is refractory to medical management without deformity
Temporary relief at most, with a 30% to 50% recurrence
Synovectomy with tendon relocation
ii) Synovectomy plus tendon relocation
May be useful for the early stages of disease, in which there is preserved joint cartilage and for refractory synovitis with ulnar displacement of extensor mechanism
Technique
Radial arthrotomy parallel to extensor tendon
Separate tendon from capsule and perform synovectomy as necessary
Partial or full release ulnar collateral ligament and ulnar intrinsic wing of extensor hood
Plicate radial collateral ligament (RCL)
Repair dorsal capsule and use “Vest over pants” repair of extensor hood
Reinforce the repair with slip of extensor tendon through the capsule.
Postoperative management
Dynamic extension splint for 6 weeks
Hand therapy
Joint arthroplasty
iii) Arthroplasty of the MP joints
Most common surgical treatment for the MP joints
Current implant materials include silicone, metal and plastic (poly ethylene)
Surgical techniques are similar
Surgical exposure
Skin incisions can be transverse or longitudinal.
Longitudinal may allow better wound healing, earlier mobilization, and preservation of dorsal venous structures.
Radial paratendinous arthrotomy with release of collateral ligaments from metacarpal head.
Synovectomy.
Trial reduction implant for sizing and need for additional soft tissue releases.
Ulnar sagittal band
Ulnar intrinsic wing at base of proximal phalanx
Abductor digiti minimi release (direct visualization to avoid ulnar digital nerve injury) at base of small finger proximal phalanx
Volar plate release as needed
Insert definitive prosthesis, tend to larger sizes for stability and longevity.
Repair RCL with correction of ulnar deformity.
Vest over pants repair of tendon, MCP capsule with centralization of extensor hood and dorsal capsule.
Skin closure with nonabsorbable suture and splint.
iv) Soft tissue balance
Critical to a successful outcome
Attention to ulnar releases, volar releases, and correct implant sizing
Repair of RCL
Protection postoperatively for 6 weeks in dynamic extension splint, active hand therapy for active and passive range of motion (ROM) of MP and interphalangeal (IP) joints
v) Long-term results
Patient satisfaction 38% at 14 years follow-up.
Substantial reduction in pain, improvement in function and appearance.
Level 2 prospective evidence proving marked and significant improvement for RA patients with poor baseline functioning treated with MCP joint arthroplasty over control medical management group at early follow up.
vi) Silicone implants: Failures occur due to
Fracture of implant at junction of hinge and distal stem, may not result in clinical failure
Long-term stability occurs from encapsulation of the implant with scar tissue
Particulate silicone synovitis
Stretching and deformation of the implants without fracturing secondary to reoccurrence of soft tissue imbalance
Joint arthrodesis
Interphalangeal joints
Bone changes
Typical of other joints in arthritis with joint destruction, deformity, and stiffness
Soft tissue deformities
Swan neck and boutonnière deformities can be seen in the same hand, different digits
Clinical issues
Despite the deformities, most are well tolerated by patients.
Symptoms related to stiffness, inability to grip. Pain can also be a problem with advanced disease.
Management: Depending on the severity of the deformity, fixed or nonfixed
Options include
II. Seronegative Arthritis
‘Seronegative’ is defined by the absence of rheumatoid factor (RF) in the blood. In some classification schemes, any arthritis in which RF is not present is classified as seronegative arthritis, including RF negative RA, osteoarthritis, infectious arthritis, gout, and others. However, seronegative usually indicates seronegative spondyloarthropathies including Psunatic arthritis (PsA), ankylosing spondylitis, reactive arthritis (Reiter syndrome), and enteropathic arthritis (the arthritis of inflammatory bowel disease). PsA is the most common seronegative spondyloarthropathy that involves the hands, and the primary focus of this section. In addition, there is a discussion of systemic lupus erythematosus (SLE) and scleroderma as they also commonly affect the hands.
Epidemiology
As a group, the seronegative spondyloarthropathies affect men more often than women, although PsA affects men and women equally.
Like the other seronegative spondyloarthropathies, the prevalence of PsA has a positive correlation with the prevalence of the HLA-B27 MHC class II allele, which varies widely between ethnic groups.
The prevalence of psoriasis in the general population ranges from 0.1% to 3%.
About 7% of patients with psoriasis develop PsA.
Pathogenesis
HLA-B27 is one of many possible alleles that can occupy the “B” locus in the major histocompatability complex on chromosome 6. The HLA molecule presents antigens to T-cells and helps launch the immune response. The exact role of HLA-B27 in the seronegative spondyloarthropathies is not well understood.
An environmental trigger is probably required to initiate the arthritis. In the case of reactive arthritis (formerly known as Reiter syndrome), the trigger is an extra-articular bacterial infection (Chlamydia, Salmonella, and others). The possible role of bacterial infection in reactive arthritis is being investigated, although the environmental triggers are not known.
Presentation
Ankylosing spondylitis, reactive arthritis, and enteropathic arthritis typically have axial involvement and asymmetric oligoarticular lower extremity joint involvement. Enthesitis and sacroiliitis are common. In addition, there are usually extra-articular findings.
Reactive arthritis: Urethritis, conjunctivitis, and prior extra-articular infection (Chlamydia, Salmonella, Yersinia, Campylobacter, or Shigella).
Enteropathic arthritis: Inflammatory bowel disease (Crohn or ulcerative colitis).
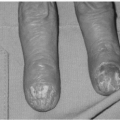
PsA presents with cutaneous findings prior to arthritis in 85% of patients. Of the 15% that develop arthritis first, all will eventually develop a rash or typical nail changes (pitting or crumbling).
PsA has five patterns of joint involvement. These patterns often overlap, and can change over time in a given patient.
Distal interphalangeal (DIP) joint arthritis
Arthritis mutilans of the digits (severe, aggressive polyarticular arthritis)
Symmetric polyarthritis indistinguishable from RA
Asymmetric oligoarthritis, often involving the hands
Spondyloarthropathy
Erosion of the terminal phalanges can occur at the tufts (acral osteolysis).
At the DIP joint, proliferation at the base of the distal phalanx combined with erosion and tapering of the middle phalanx can result in a “pencil-in-cup” deformity.
DIP ankylosis is common.
Aggressive osteolytic changes seen with arthritis mutilans can result in an “opera glass hand” with collapse of the digits.
Psoriatic dactylitis, with fusiform swelling due to periostitis, tendonitis, and enthesitis can occur.
Unlike in RA, hand deformities tend to be asymmetric.
The most common finger deformity is a flexion contracture of the proximal interphalangeal (PIP) joint with secondary hyperextension of the metacarpophalangeal (MP) joint.
Swan neck deformities do occur, and usually initiate with a mallet finger.
The MP joints tend to develop extension contractures.
In the thumb, MP flexion and IP extension contractures are common.
Wrist involvement is common.
Diagnosis
There are no specific diagnostic criteria for PsA. The diagnosis is made when there is an inflammatory seronegative arthritis with axial or asymmetric peripheral involvement, in the setting of psoriatic skin lesions or typical nail changes.
Imaging
Acral osteolysis with resorption of distal phalangeal tufts, spontaneous DIP ankylosis, and the pencil-in-cup deformity are common radiographic findings. Sacroiliitis is also seen.
Nonsurgical treatment
NSAIDs are used to treat early disease, but may make cutaneous lesions worse. Other medications similar to those used to treat RA may be used (methotrexate, cyclosporine, sulfasalazine, gold salts, antimalarials, and azathioprine).
Surgical treatment
Surgical treatment of wrist and finger deformities is often necessary to treat pain and improve function.
Painful PIP joint with severe articular destruction (and bone defects) or PIP flexion deformities that are fixed can be treated with arthrodesis to relieve pain and place the joint in a more functional position.
Swan neck deformities may require surgery to improve function and should be approached like a rheumatoid swan neck deformity.
Silicone arthroplasty is often necessary to correct extension contractures (and occasionally flexion contractures) of the MCP joint.
The DIP joints rarely require arthrodesis due to the high rate of spontaneous ankylosis.
In cases of arthritis mutilans, arthrodeses with bone grafts to restore length are required.
In the thumb, MP or IP arthrodesis is often necessary. Carpometacarpal (CMC) arthritis is treated with resection arthroplasty and ligament reconstruction to relieve pain preserve motion.
In the wrist, limited or complete arthrodesis is sometimes indicated for pain. Distal ulna resection or Sauve-Kapandji procedure can be used when the DRUJ is involved.
Other connective tissue diseases involving the hands
SLE and scleroderma are two common connective tissue diseases that often affect the hands. RF is present in 20% to 30% of patients with these conditions, although most are seronegative for RF.
SLE is a multisystem inflammatory disease affecting the skin, heart, lungs, kidneys, and periarticular soft tissue. About 85% of patients have cutaneous findings, including a butterfly rash on the face, or an erythematous maculopapular rash on the palms and fingers, both of which tend to occur after sun exposure. Patients are usually young females. SLE is more common in African Americans than whites.
There are a number of changes that commonly occur in the hands.
Raynaud phenomenon.
Morning stiffness that improves with motion.
Symmetric hand joint involvement, with swelling and pain.
Hand deformities are very similar to those seen in RA (ulnar translocation of the carpus, radial deviation of the metacarpals, ulnar deviation of the fingers, volar subluxation of the MP joints, swan-neck and boutonnière deformities of the fingers). However, in SLE they are due to soft tissue pathology only, without articular involvement.
X-rays do not show osseous or articular changes consistent with arthritis.
Early in the disease, passively correctible deformities are best managed with therapy and splinting to preserve function. Surgery is indicated to improve function in patients that do not improve with nonsurgical management.
Soft tissue reconstruction alone has a high failure rate.
2) In spite of a lack of articular changes, arthrodeses or arthroplasties are often performed in combination with soft tissue reconstruction to prevent recurrence.
Common operations include
Limited or total wrist arthrodesis for instability or ulnar translocation.
The Darrach procedure (distal ulna resection) or Sauve-Kapandji procedure for dorsal subluxation of the ulna and arthritis of the DRUJ.
MP silicone arthroplasty combined with soft tissue reconstruction for ulnar deviation and volar subluxation. For the thumb MP joint, arthrodesis is preferred.
PIP joint arthrodesis.
Scleroderma is a multisystem disease that affects the skin, kidneys, heart, lungs, and GI tract, resulting in progressive fibrosis of connective tissue. It is more common in females than males (4:1).
There are three clinical patterns.
Diffuse scleroderma: Widespread skin hardening and multiple organ system involvement.
Limited scleroderma (CREST): Skin hardening limited to hands and face—Calcinosis, Raynaud phenomenon, Esophageal involvement, Sclerodactyly, Telangiectasias.
Linear (morpheaform): Isolated small areas of skin hardening without systemic involvement.
Hand symptoms and deformities are common and diverse.
Raynaud phenomenon is very common.
Fingertip ulceration and autoamputation can occur.
Ulceration is common over the convex surface of contractures.
Cutaneous fibrosis leads to contractures in the fingers and loss of function. PIP flexion contractures with compensatory MP hyperextension are the most common deformities. Tendon rupture and skin breakdown often occur with these contractures.
First web space contracture is common.
X-rays may show tuft resorption.
Cutaneous or subcutaneous calcinosis in the fingers can occur and can be painful.
Therapy and splinting rarely slow the progression of the disease. Surgery is indicated primarily to improve function and to treat nonhealing wounds or infections, such as osteomyelitis. The decision to operate should be made carefully, since patients with scleroderma heal poorly and are prone to infection.
Nonhealing ulcerations over joints contractures may require resection of bony prominences or arthrodesis.
Symptomatic calcinosis can be treated with resection, debulking, or curettage.
Distal amputation may be necessary for nonhealing wounds associated with osteomyelitis.
Circulation must be carefully assessed prior to surgery, particularly distal to the middle phalangeal level.
Medications such as calcium channel blockers may improve distal circulation.
Fixed PIP flexion deformities should be corrected with arthrodesis, including enough bone resection to ensure adequate soft tissue coverage.
Fixed MP contractures are treated with resection arthroplasty. A volar approach will allow less tension on the wound closure if it is an extension contracture.
First web space soft tissue release is commonly performed to improve grasp. Thumb MP or IP fusion may improve pinch in some patients. CMC resection arthroplasty with ligament reconstruction may be helpful to improve thumb motion.
III. Crystalline Arthropathies
Definition
Gout is a disorder of urate metabolism that results in high levels of uric acid in the blood, urine, and synovial fluids. Under certain conditions, urate crystals precipitate within the joint and synovium resulting in inflammatory arthritis.
Pseudogout, one manifestation of calcium pyrophosphate dihydrate (CPPD) deposition disease, is a disorder in which CPPD crystals precipitate within the joint or synovium resulting in acute inflammatory arthritis.
Epidemiology
Gout affects 1 % to 2% of the general population, and is more common in males and African Americans. It most commonly presents in men in their fourth to sixth decades of life, and for women in their sixth to eighth decades. Risk factors include age, family history, heavy consumption of alcohol, meat or seafood, diuretic use, obesity, and renal failure.
Pseudogout or CPPD is common in the elderly. The prevalence of CPPD is 10% to 15% in the sixth and seventh decades, and increases to 40% in those over 80. Risk factors include age, family history, hyperparathyroidism, and hemochromatosis.
Pathogenesis
Hyperuricemia (serum uric acid > 6.5 mg/dL) is common and usually asymptomatic. Some patients, however, with hyperuricemia can develop precipitation of sodium urate crystals in the joints and soft tissues, leading to localized inflammation. Changes in tissue pH, temperature, or hydration can affect the solubility of uric acid and lead to crystal precipitation. Certain drugs, notably cyclosporine, can also result in gout.
The pathogenesis of CPPD is not well understood. CPPD crystals are deposited in and around the joint, particularly on the cartilage surfaces, resulting in inflammation. The increased deposition of CPPD is due to high local concentrations of calcium or pyrophosphate, and altered intracellular and extracellular metabolism of pyrophosphate.
Presentation
The natural history of gout progresses through four clinical stages.
Asymptomatic hyperuricemia
Acute gouty arthritis
Intercritical gout (periods between acute attacks)
Chronic tophaceous gout
Acute gout occurs most often in the lower extremities, and is usually monoarticular or oligoarticular.
The first metatarsophalangeal joint is most often involved (podagra).
Involvement of other joints in the feet, ankles, and knees is common.
Symptoms include acute severe pain, erythema, and swelling.
Acute attacks last about a week, but can range from a few days to a few weeks.
Fever and leukocytosis may be present with acute attacks, particularly in patients with chronic polyarticular gout.
Upper extremity involvement is less common than lower extremity involvement, and is more frequent in older patients with underlying chronic gout. It may involve the wrist, MCP joints, or IP joints. If acute gouty arthritis presents in the wrist, it can mimic exactly the presentation of septic arthritis.
Involvement of the IP joints occurs more commonly in older patients, and is more common in women with gout. It may affect sites of prior osteoarthritis, and inflammation of Heberden or Bouchard nodes is often present. This is often the presenting symptom in late-onset gout in females.
Chronic tophaceous gout is due to recurrent bouts of acute gout. Soft tissue deposits of sodium monourate crystals (tophi) develop, commonly at the IP joints in the hand and over the olecranon process. Periarticular and intraosseous tophi cause joint destruction and deformity over time. Chronic tophaceous gout may be punctuated by attacks of acute, often polyarticular gout.
Acute pseudogout causes joint swelling, pain, and erythema, and feels similar to a gout attack. It may last from days to weeks if untreated. It is usually monoarticular and most commonly involves the knee or other large joints like the hip, shoulder, and wrist. Chronic CPPD deposition disease in the upper extremity usually presents as a chronic arthropathy, resulting in cartilage calcification (chondrocalcinosis) and degenerative changes in the joint. It usually affects the wrist and MCP joints symmetrically, with relative sparing of the IP joints.
Diagnosis
Gout is often diagnosed clinically, particularly if classic podagra or tophi is present. In their absence, laboratory studies may aid in diagnosis.
Most patients have chronic hyperuricemia (>6.5 mg/dL), although urate levels may be normal during an attack, or may be elevated in the absence of gout.
Definitive diagnosis is made by arthrocentesis.
Monosodium urate (MSU) crystals are negatively birefringent under a polarized light microscope, and are thin, long, and pointed.
The crystals may be intracellular or extracellular.
Crystals may also be identified in tophi.
White blood cell counts (synovial fluid) are usually in the inflammatory range, from 10,000 to 20,000 WBC per µL.
Acute pseudogout may be suspected with the appropriate clinical presentation (acute monoarticular inflammatory arthritis, particularly of the knee), but definitive diagnosis is made with arthrocentesis.
CPPD crystals are positively birefringent under a polarized light microscope, and are shorter and less sharp tipped than MSU crystals.
Crystals may be intracellular or extracellular.
White blood cell counts (synovial fluid) are in the inflammatory range, from 10,000 to 20,000 per µL.
The diagnosis of chronic CPPD deposition disease is usually made clinically and radiographically, although identification of crystals may confirm the diagnosis.
Septic arthritis should always be considered in the differential diagnosis, and is discussed later in this chapter. Cell count, Gram stain, and cultures should be preformed on all arthrocentesis specimens in cases of suspected gout or pseudogout.
Imaging
Routine radiographs are not particularly useful in diagnosing acute gout or pseudogout. They should be obtained, however, to identify chronic changes or other pathology, and to serve as a baseline. In chronic tophaceous gout, articular and periarticular tophi cause metaphyseal and subchondral erosions on both sides of the joint in question, typically with sclerotic borders and overhanging margins. Joint space narrowing and destruction are late findings. Chronic CPPD deposition leads to chondrocalcinosis seen as dense linear calcifications at the articular surface, and accelerated degenerative joint changes. In the wrist, a pattern of collapse similar to scapholunate advanced collapse (SLAC) is common. Other imaging modalities such as CT, MRI, and ultrasound are not routinely used in the diagnosis of acute gout or pseudogout, although their potential roles are being studied.
Nonsurgical treatment
A rheumatologist should be consulted to assist in the management of acute or chronic tophaceous gout, or acute pseudogout.
Acute gout is treated with NSAIDs, colchicine, or corticosteroids.
Indomethacin (an NSAID) is traditionally used for acute gout, but caution should be used in older patients and those with compromised renal function.
Colchicine is very effective in stopping an acute gout attack, although it has many potential side effects, and caution should be used in older patients.
Corticosteroids are becoming more popular in the treatment of acute gout, particularly in patients with contraindications to colchicine or NSAIDs. They can be administered as an intra-articular injection or systemically.
Patients with chronic tophaceous gout or recurrent acute attacks benefit from urate lowering (hypouricemic) drugs.
Probenecid is a hypouricemic drug that increases urate excretion in the urine (uricosuric drug) thereby lowing serum levels. A side effect of probenecid is nephrolithiasis.
Allopurinol is a hypouricemic drug that acts by inhibiting xanthine oxidase.
Joint rest, NSAIDs, and intra-articular corticosteroid injections are the primary treatment modalities for acute pseudogout. Colchicine may also be helpful in an acute attack, but is used infrequently because of its side effects.
Surgical treatment
There is little role for surgery in treating acute gout or pseudogout. Surgery is sometimes indicated in chronic tophaceous gout, or in chronic CPPD deposition disease.
Tophi.
In general, soft tissue tophi should be treated medically, due to the risk of infection and poor healing after surgical excision.
Irrigation and aspiration using large-bore needles inserted through uninvolved skin have been described, and may be used to reduce symptomatic soft tissue tophi.
Osseous tophi that threaten the joint should be curetted and bone grafted.
Painful or unstable joints with significant articular destruction due to gout may be treated with arthrodesis.
CPPD deposition disease is a common cause of SLAC-pattern degenerative wrist collapse in older patients. SLAC operations such as proximal row carpectomy (PRC) or scaphoidectomy and four-corner arthrodesis may improve pain. Painful degeneration of the MP joints due to CPPD deposition can be treated with arthrodesis or arthroplasty.
Other crystalline arthopathies
A group of calcium-containing molecules called basic calcium phosphate (BCP) crystals have been implicated in the pathogenesis of osteoarthritis. Because BCP crystals cannot be seen under polarized light microscopy and are difficult and expensive to accurately identify, their role in the development of osteoarthritis or other arthritides is not well understood.
IV. Infectious Arthritis
Definition
Septic arthritis is commonly caused by pyogenic bacteria in the joint, usually at concentrations greater than 100,000 organisms per mL. Less common culprits of septic arthritis include mycobacterial and fungal organisms.
Epidemiology
The incidence of septic arthritis is about 0.002% in the general population. It is more common in immunosuppressed patients and in patients with prosthetic joints (0.05%).
Pathogenesis
Septic arthritis may occur as a result of direct introduction of bacteria into a joint by a penetrating object, or by spread of an adjacent infection such as cellulitis or osteomyelitis. More commonly, it is due to hematologic seeding.
In the case of direct introduction of bacteria, Staphylococcus aureus followed by streptococcal species are the most common causative organisms. Coagulase-negative Staphylococcus is the most common organism in prosthetic joint infections. Gram-negative, anaerobic, or mixed infections occur in heavily contaminated wounds or in immunocompromised patients.
Hematogenous seeding is most common in immunocompromised patients, diabetics, dialysis patients, IV drug users, patients with endocarditis, and patients with indwelling catheters.
Other common clinical scenarios include
Pseudomonas or Candida infections in IV drug users.
Salmonella infections in patients with sickle cell anemia.
Group B streptococcal infections in infants and children under 5 years of age.
Eikenella corrodens infection in human bites (fight bites of the MCP joint).
Pasteurella multocida infection from animal bites, particularly cat bites.
Salmonella infection after rodent bites.
Rarely, atypical mycobacterial or fungal infections may occur.
Presentation
Patients present with acute inflammation of a single joint, including pain, edema, erythema and loss of motion. Systemic signs and symptoms such as fever and leukocytosis may be seen. Other risk factors such as a direct injury, IV drug use, or an indwelling catheter may be present.
Diagnosis
History should be taken to assist in determining the source of infection.
Physical examination reveals severe pain with active or passive ROM and with gentle axial loading of the joint.
Laboratory studies including a CBC with differential, ESR, CRP, and blood cultures should be obtained.
Definitive diagnosis is made by arthrocentesis.
Fluid should be sent for cell count and differential, Gram stain, and cultures (aerobic and anaerobic).
If there is enough fluid, it should be sent for crystal studies, and protein and glucose levels.
If indicated, fungal and mycobacterial stains and cultures should be ordered.
WBC counts range from 50,000 to 300,000 per µL. Lower counts with a high percentage of PMNs may also suggest infection.
A glucose level of 40 mg/dL, or less than the fasting blood glucose level, also suggests infection. However, synovial glucose and protein levels are rarely helpful in diagnosis due to their low sensitivity and specificity.
Imaging
Routine radiographs should be obtained and examined for foreign body, gas, or signs of osteomyelitis. Initially radiographs show a widened joint space due to intra-articular edema and purulence. Joint space narrowing and articular erosions are late findings.
Treatment
Septic arthritis is a joint-threatening emergency, and is managed with urgent drainage and IV antibiotics. Antibiotics are not usually initiated until fluid has been obtained for cultures.
The septic joint should be treated with arthrotomy, drainage, and irrigation.
The joint capsule should not be completely closed, and a drain or wick should be placed to allow for continued drainage. Articular cartilage should not be exposed to dessication.
The skin should be closed very loosely or not at all.
Postoperative saline wet to dry dressing changes should be performed, with TID warm soaks in dilute hydrogen peroxide or iodine solution.
Active and passive ROM should be initiated early on to prevent stiffness.
If there is no improvement within 24 hours, or if purulent drainage persists, repeat washouts are indicated.
Arthroscopic washout of the radiocarpal joint is an alternative to open drainage.
Empiric IV antibiotics are initiated as soon as a diagnostic aspiration has been performed. A broad-spectrum antibiotic, which will cover Gram-positives, Gram-negatives, and anaerobes, should be used initially. The antibiotic coverage can be narrowed based on Gram stain and culture results. IV antibiotics should be continued for 2 weeks, followed by oral antibiotics to complete a 4 to 6 week course.
V. Juvenile Idiopathic Arthritis
The International League of Associations for Rheumatology (1997) has recently changed the classification of chronic arthritis in children under 16 years of age to Juvenile Idiopathic Arthritis. JIA is what was classically referred to as Juvenile Rheumatoid Arthritis and includes other types of chronic inflammatory arthritis. Though, there are some similarities amongst the juvenile and adult forms, the change in terminology more accurately reflects the difference between the childhood diseases and those chronic arthritides afflicting adults.
I. Classification
Systemic
Polyarticular
RF positive
RF negative
Oligoarticular
Persistent
Extended
Psoriatic
Enthesitis related
Other
Systemic
Incidence: 10% to 20%.
Mean age of onset of 5.
Males and females are equally afflicted.
RF and ANA are usually negative.
Many extra-articular manifestations.
High spiking fever
Anemia
Macrophage activation syndrome
Polyarticular
Involves five or more joints
RF negative
Incidence: 20% to 30%
Mean age of onset 3 years, early childhood
Females are more afflicted than males
ANA positive in 25%
Variable prognosis
RF positive
Incidence: 5% to 10%.
Mean age of onset late childhood, adolescence.
Females are more afflicted than males.
ANA positive in 75%.
Small joint involvement
Boutonnière deformities
Swan neck deformities
Oligoarticular
Incidence: 50% to 60%
Large joint involvement: Knee and ankle
Less than five joints involved during first 6 months
ANA positive 50%, elevated ESR
Subtypes
Persistent
Arthritis confined to four or fewer joints
Better prognosis
Extended
3. Arthritis of five or more joints after 6 months
4. Worse prognosis
PsA
Incidence: 2% to 15%
Peak age mid childhood
Asymmetric arthritis
Musculoskeletal involvement
Knees and ankles
PIP, DIP and tendon sheaths
Sausage digits
Extra-articular
Rash
Nail changes
Uveitis
Enthesitis Related
Incidence: 1% to 7%
Includes ankylosing spondylitis
Inflammatory bowel disease associated arthritis
HLA-B27 associated
Males predominantly affected
Age greater than 8
Hallmarks
Pain and stiffness
Low back pain
Uveitis
RF and ANA negative
II. Diagnosis
Clinical findings
Hand
Joint swelling
Dactylitis
Nail changes
Orthopaedic
Joint swelling
Inflammatory lumbosacral pain
Sacroiliitis
Systemic
Rash
Fever
Serositis
Joint aspiration
Turbid yellow fluid
WBC 5,000 to 8,000.
Blood testsRelated posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree