Fig. 20.1
The main structure of the expander
1.2.1 Expander Capsule
The expander capsule is the main part of the expander, and its main function is to receive the injected water to complete the expansion of the skin tissue; thus, it is required that the expander capsule itself not only has better elastic scalability and good leakproofness but also has strong blast-resistant and tear-resistant abilities and can receive the injected water over the rated capacity for expansion. According to the shapes of the expander capsules, the expanders can be divided into several types of round, square, kidney-shaped, cylindrical, and special-shaped expanders (Fig. 20.2), and each type has different capacity specifications.
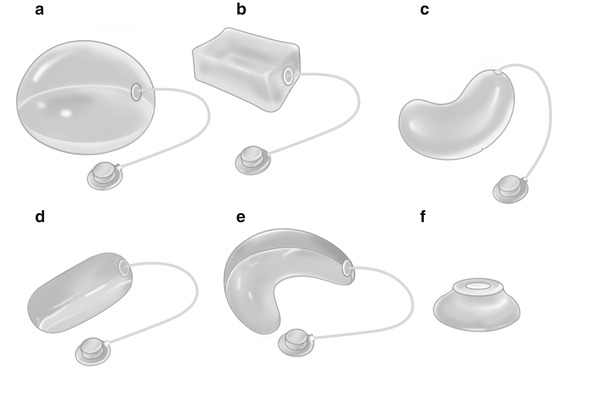
Fig. 20.2
The expander capsules with different shapes. (a) Round. (b) Square. (c) Kidney shaped. (d) Cylindrical. (e) Crescent shaped. (f) Top injectable type
- 1.
Round expanders. They include spherical, hemispherical, elliptical, and pie-shaped expanders, which have capacity specifications of 30, 50, 100, 140, 300, and 500 ml. This type of expanders after expansion can make the skin surface hemispherical, the central expansion rate was highest, and it can be used in various parts of the body, of which, during breast reconstruction process, the saline-filled prosthesis is also a round expander.
- 2.
Square expanders. They include rectangular, cubic, and ice bag-shaped expanders, which have capacity specifications of 100, 170, 250, 500, and 700 ml. The skin flap formed after the expansion of the square expander capsule is easy to be slided and advanced forward and backward, and thus they are mostly used in the trunk and limbs.
- 3.
Kidney-shaped expanders. The kidney-shaped expander capsules have capacity specifications of 20, 30, 50, 100, 250, and 450 ml. The skins expanded by this type of expanders are bulged as kidney shaped, the inner radian is smaller, and the outer radian is larger, and thus the skin expansion rate is higher, and they are mostly used in parts matching the radians, such as mandibular margin, neck, infraorbital area, and retroauricular area.
- 4.
Cylindrical expanders. They include cylindrical and semicylindrical expanders, which have capacity specifications of 10, 100, 200, and 400 ml; they are mainly used for the expansion of the limb skin.
- 5.
Special-shaped expanders. The expander capsules are designed according to special parts or special needs, such as C-shaped expander used in periorbital area, horseshoe-shaped expander used in mandibular area, and long strip-shaped expander used in dorsal side of fingers.
1.2.2 Injection Pot
The injection pot is the major component which receives puncture and injects the expansion solution into the expander capsule, and the main structures include top cover, bottom cover, anti-puncture stainless steel sheet or nylon sheet, and anti-leakage device. The valves can be divided into unidirectional valve and bidirectional valve according to whether limiting the flow direction of the expansion solution. Because the unidirectional valve only allows the flow of the expansion solution from the injection pot to the expander capsule, although it can effectively prevent valve leakage, but once the excessive injected water leads to the blood supply disorder of the expanded skin, the treatment will be more difficult, the bidirectional valve is mostly used in domestic hospitals, and the advantage is that the intracapsular pressure can be adjusted through injecting or drawing out the expansion solution.
Another kind of external water injection valve has a similar principle with the built-in valve, but the injection pot is placed externally during surgery. Some expanders are still designed with flapper type valve, which is connected to the end of the aqueduct; after the front-end nipple of the syringe is inserted into the valve, the valve can be opened immediately for water injection.
1.2.3 Aqueduct
The aqueduct is the silicon tube connecting the injection valve and expander capsule, the length is about 5–15 cm, and the diameter is generally 2.0–3.5 mm. The tube walls generally have a certain thickness, so as to avoid being flattened, twisted, and folded.
Over the years, with the widely application of expanders in clinic, some domestic scholars have also carried out continuous improvement on the expander, so that it can be better applied in clinic or research. For example, Li Jiang et al. developed the thin-walled vertical tube expander; because the tube is perpendicular to the long axis of the expander, the injection pot is separated from the tube; it can be implanted under the skin through minimally invasive surgery, while the use of an external injection pot avoids problems of expander tube folding and injection pot leakage; its clinical application has achieved better results. Liu Wenge et al. developed the expander with structures such as double capsules and double tubes; its external capsule is used to store the drug solution promoting the expansion; the internal capsule is used for water injection and expansion, and the expansion time is reduced through combined use of the drug solution, so that the expansion efficiency is greatly improved. Jiang Huiqing et al. developed the polyester mesh unidirectional expander. The strength of the bottom is increased, and the expander produces a unidirectional expansion effect, which is more favorable for the expansion of cervical and abdominal skins. Lu Yanlin et al. modified an expander; the aqueduct is fixedly connected with the injection valve, and the aqueduct and expander capsule are produced separately; the length of the aqueduct is up to 100 cm; when being used, it can be cut short according to actual need, and then it is bonded together with the expander capsule using adhesives, so that the distance between the implanted expander capsule and the injection pot is increased, reducing the incidence rate of infection when the injection pot is placed externally [10].
1.3 Surgical Steps
1.3.1 Expander Implantation
The expander implantation is the first-stage surgery we often mention.
- 1.
Selection of expansion area. The expanders with different shapes are selected according to characteristics of the defect areas to be repaired; the area where the expander is implanted is generally selected in the area adjacent to the lesion area; in this way, the color and texture of the expanded skin are most similar to the area to be repaired; thereby, an excellent postoperative aesthetic effect is obtained. The situation such as scarring, trauma, or infection should be avoided in the proposed expansion area, so as not to cause infection or exposure after expander implantation. At the same time, consideration should be given to the blood supply situation of prefabricated skin flap in the implantation site of the expander; the proposed expansion area should be far away from the sites where the main supplying vessels of the skin flap penetrate out; especially when the expander is implanted in the limbs or trunk, attention should be paid to retaining the longitudinal blood vessels in line with the direction of the skin flap expansion, while the unnecessary transverse blood vessels are cut off, so as to achieve the effect of skin flap delay. Selecting the appropriate expansion area is the guarantee of the surgical efficiency, and the placement location and direction of the expander have an important impact on the skin expansion efficiency. According to the study of Fan Pengju et al., because the skin has anisotropy in the expansion process, the expansion efficiency is lowest along the direction of Langer’s lines, and the expansion efficiency is highest along the direction perpendicular to Langer’s lines; at the same time, the non-round expander also has different expansion potential energies in all directions; the expansion efficiency in its long axis is often not as good as that in its short axis [11]. This suggests that when the expander is implanted, the plastic surgical surgeons should not only consider the skin situation of the patient but also comprehensively consider the expansion characteristics of the surrounding normal skin and the shape of the pre-implanted expander and the expansion potential energies in all directions.
- 2.
Incision selection. The intraoperative incision design needs to consider the factors such as the site, size, direction, and tension of the incision; the first-stage surgery also needs to consider the location of auxiliary incision in the second-stage surgery and how to transfer the skin flap, in order to take full advantage of the expanded tissues and provide favorable conditions for the second-stage surgery. The principle of skin flap design should be run through the entire surgical procedure.
The incision for expander implantation is usually selected in the place at the junction of diseased tissue and normal tissue, which is beneficial to wound healing, and can effectively prevent complications such as incision dehiscence and expander exposure. However, some scholars believe that the incision made in the normal skin side of the junction can affect the skin expansion efficiency; it is recommended to make the incision in the affected skin, but the margins of the implantation lacuna of the expander are dissociated underneath at least to the normal skin side; the isolation strip between the expander and the incision is established, which can take advantage of the normal skin without the formation of a new scar, and simultaneously ensure that the wound healing is not affected by the tensile force of the expander. For the selection of incision direction, the incision which is parallel or perpendicular to the long axis of the expander is used in most cases, so as to facilitate separating the subcutaneous lacuna. It is appropriate that the length of the incision is enough to fully separate the lacuna and doesn’t exceed the lesion range. Some scholars believe that the straight incision made in the place at the junction of affected skin and normal skin is not conducive to the expansion of the skin flap; they suggested that the small V-shaped or U-shaped incision is made at the side of the affected skin, or the incision should be made perpendicular to the direction of the skin flap expansion. Some researchers have compared the advantages and disadvantages of the parallel incision and vertical incision and have found that the visual field exposure of the vertical incision is poor, and the dissection difficulty is greater and thus is not conducive to hemostasis. But as long as the operation is performed carefully during surgery, because its incision tension is perpendicular to the tension expanding the skin soft tissue, the postoperative complications such as wound dehiscence are significantly reduced, and the skin expansion efficiency is also significantly increased [12].
For some banded pigmented nevi or melanin hairy nevi, the affected skin can also be selected as the center to make the incision; the expander is implanted to expand the surrounding skin; after the expander is taken out at the second-stage surgery, the banded affected skin is removed, and the incision is directly sutured. Because when the water injection and expansion are carried out after surgery, the tension born by the incision is greater, for this type of incision, during surgery, the dermis and subcutaneous tissue should be incised at one side of the incisal margin, and then the clearance of the expansion capsule is stripped; when the incision is closed, the formed deep dermal flap should overlap into the subcutaneous area and is tiled with it to reinforce the incision.
With the popularization and application of endoscopy in plastic surgery, more and more hospitals begin using the expander implanted by minimally invasive surgery, so that the first-stage incision is smaller and smaller. Under the condition that the safe hemostasis is achieved, the appropriate implantation lacuna is separated, and the expander capsule is fully flattened; the smaller incision heals more quickly after surgery, so that the expansion cycle is shortened, and the expansion efficiency is improved. The use of endoscope for expander implantation has advantages such as shorter operative time, small incision, faster recovery, fewer complications, and better postoperative effect and thus is highly respected by plastic surgeons [13].
- 3.
Implantation depth. The implantation depths of the expander in different parts of the body are not the same; for example, for scalp expansion, the expander is generally implanted into the surface of the skull periosteum at the deep surface of the galea aponeurotica; for expansion of the facial buccal skin, the expander is generally implanted into the deep surface of the subcutaneous tissue and superficial surface of SMAS layer; for cervical skin expansion, the expander is generally implanted into the superficial or deep surface of the platysma muscle, but it is generally believed that the expander should be implanted into the superficial surface of the platysma muscle, because the separation operation of the deep surface of the platysma muscle may damage the cervical branch of the facial nerve; for the expansion of the skin in the trunk and limbs [14], the expander is generally implanted into the superficial surface of the deep fascia.
- 4.
Lacuna separation. The implantation lacuna of the expander is mainly separated by means of blunt dissection; the interval in the site connected more closely can be cut off with scissors, but attentions should be paid to strict hemostasis. The separation operation should be located in the same tissue layer, to avoid that the uneven thickness of the skin flap at the surface layer causes the expander exposure in the future expansion process [15]. The size of the lacuna should exceed the margin of the flattened expander capsule by about 1 cm; if the lacuna is too small, it may lead to the fact that the expander is folded into a corner and pierces the skin. The lacuna where the injection pot is placed cannot be too close to that of the expander capsule, so as not to cause accidental injury of the expander capsule when the water injection is carried out.
- 5.
Expander implantation and incision closure. Before expander implantation, the leakproofness of the expander should be strictly examined to ensure that no damage occurs; 10–20 ml normal saline or gas can be injected into the expander, and then the expander is placed into the water to inspect whether there is leakage. After complete hemostasis of separated lacuna, the expander is prefilled with a certain amount of normal saline (generally 10–20% of total capacity) to fully expand and flatten the expander within the lacuna. When the injection pot is placed, it should be noted that the injection surface is placed upwards to avoid its overturn and the tube folding. Before incision closure, a negative pressure drainage tube is placed at the bottom of the lacuna to facilitate postoperative drainage.
When the incision is sutured, the superficial tissue should be sutured with the deep tissues with several stitches at the 0.5–1 cm from the incisal margin, so as to prevent the translocation of the expander to the incisal margin in the process of water injection and expansion, which causes great tension on the incision and affects wound healing and even leads to expander exposure. After that, the incision is closed by means of layered intermittent suture, and the entire process must be carried out under direct vision to prevent piercing the expander. After completion of the suture, the injection pot can be punctured for water injection test to ensure that injection pot is not overturned. The negative pressure drainage tube is connected to the negative pressure suction machine for examination to ensure tight incision suture.
With the universal application of the expander and the continuous improvement of its structure, in recent years, the implantations of the expanders with external injection pot are also continuously increased. Relative to the expander with built-in injection pot, the external injection pot gets the favor of surgeons because of its easy operation, no need for percutaneous puncture, and no occurrence of situation such as surgical failure caused by overturning of injection pot, aqueduct twist, and leakage of injection pot. In addition, the external injection pot can be converted to a special valve to be connected to other automatic water injection devices; thereby, the water injection mode is further improved, and the expansion efficiency of the skin flap is increased.
1.3.2 Water Injection and Expansion
- 1.
Conventional expansion. In general, the saline accounting for 10–15% of rated capacity is injected to the expander intraoperatively, and the water injection and expansion are carried out again at 5–7 days after surgery. The conventional expansion method is that the water injection is carried out once every 5–7 days or may be carried out twice weekly. Each injection volume is determined according to the size of the expander and the location of the expansion; generally 10–15% of the rated capacity can be injected. The isotonic saline and the isotonic solution added with antibiotics can be used as the expansion solution to prevent infection. During injection, the injection volume can be determined through the observation on the color of surface skin and the situation of capillary filling of the expanded skin flap and the simple palpation; if the surface skin becomes white after injection, and the congestion reaction disappears, the observation should be carried out for 5–10 min; if the blood flow of the skin still cannot recover to normal or the patient has an obvious pain, it is required to take some solution out until the blood flow of the surface skin is restored.
Because the conventional expansion mode of water injection has a longer interval, the entire expansion cycle is long, and there are more complications; people have always wanted to shorten the water injection cycle and increase the expansion efficiency of the skin flap. The recently developed intraoperative immediate expansion technique, the rapid expansion, and the continuous and constant pressure expansion also begin to be used in clinic and have achieved certain effects.
- 2.
Immediate expansion. The appropriate expander is implanted in the margin of the wound to be repaired; the incision is temporarily sutured; the expander capsule is injected with water immediately and repeatedly during surgery; the skin is significantly expanded after 1–1.5 h; at the moment, the expander can be taken out, and the advancement skin flap is formed to repair the wound. This expansion method can achieve the purpose of repairing the wound at a time, but it is effective only for the wound with minor defect; it is difficult to repair a large area of skin defect. Because the expansion duration is very short, all additional skins come from the elastic expansion of the tissues and the creep deformation of the tissues; there is no cell proliferation in the biological meaning; therefore, the skin flap retracts significantly after surgery; even after suture, the incision tension will be greater; and the postoperative scar hyperplasia will be obvious.
- 3.
Intermittent rapid expansion. Under the premise of ensuring no impact on the wound healing, the first water injection and expansion are carried out as early as possible; the interval between two adjacent water injections and expansions is significantly shortened compared with the conventional expansion. Generally the water injection is carried out once every 2–3 days or even once a day; each injection volume is determined according to the capacity of the expander and the area of the skin to be expanded and under the premise that the pressure produced by the expander capsule doesn’t block the skin blood flow. After water injection, the blood supply of the expanded skin flap is closely observed for 10–20 min; if the microcirculation of the skin flap is improved, some solution will be drawn out. In most cases, it takes 10–15 days to complete the entire process of water injection and expansion [16].
After rapid expansion, the reconstruction of skin structure is lower than the conventional expansion, also mainly through the elastic expansion and the creep deformation of the tissue; the proportion of cell proliferation is smaller, and the proportion of postoperative skin flap retraction is higher. But Zeng et al. compared the skin flaps undergoing conventional expansion and rapid expansion; with the extension of recovery time after water injection, the mechanical properties such as tension and retraction proportion of the skin flap undergoing rapid expansion constantly tend to be close to those of the skin flap undergoing conventional expansion; after completion of rapid water injection and expansion, the recovery time is 4 weeks; there is almost no difference in biomechanical properties between the prefabricated skin flaps with two expansion methods. It is visible that the convalescing period of the skin flap from the completion of water injection and expansion to second-stage surgery is one of key factors affecting the expanded skin flap.
- 4.
Rapid expansion with continuous and constant pressure. The implanted expander which is connected to the microelectric infusion pump in vitro via a tube is continuously perfused for expansion; the perfusion pressure is generally maintained at 5.3–8.0 kPa, and the average speed of the perfusion is 1–2 ml/h. Research shows that the continuous expansion of 6 days can obtain the volume which can be obtained through conventional expansion of 27 days; a number of indicators confirm that the increased net area is a little smaller than that after conventional expansion; the continuous and constant pressure rapid expansion is a safe and reliable water injection mode with better future prospects. The disadvantage of this method is that the water injection process requires hospitalization of the patient and requires a certain equipment to complete.
- 5.
Slow expansion. The interval between two adjacent water injections is significantly longer compared with the conventional expansion; for some sites with thinner expanded skin flap, surface scar, or radiation injury, the slow expansion can usually achieve a better efficacy, and the complication rate is usually lower.
In addition, with regard to the total amount of water injection of the expander, most researchers believe that a certain amount of over expansion is useful and harmless. Mascio et al. studied the situations such as the overexpansion of the expander and considered that it is still safer when the total amount of water injection of the expander is 3.6 times more than its standard capacity; the carefully planned overcapacity expansion can avoid multiple surgical implantations of the expander, reduce the total hospitalization cost, and obtain a better curative effect. The study of Hafezi et al. also confirmed that the overexpansion by two–four times will not increase the complication rate throughout the surgery and can provide more skin flap area to better repair the wound [17].
1.3.3 Skin Flap Transfer After Removal of the Expander
The skin flap transfer after removal of the expander is commonly referred to as the second-stage surgery.
After the skin soft tissue undergoing full expansion achieves the desired purpose, the expander can be removed, and the formed skin flap can be used to repair the defect area. It is important to note that after the completion of water injection process, it is required to maintain the expansion state of the skin flap for 4–6 weeks, so that the expanded skin flap can obtain sufficient biological extension and establish a stable and reliable blood supply, and reduce the incidence rate of complications such as postoperative skin flap retraction and blood supply disorders. Especially for some skin flaps undergoing overexpansion, the relaxation training of the skin flap can be carried out at 3 days before second-stage surgery, and the method is that 20–30% of the normal saline in the expander capsule is drawn out to make the skin flap softened; after the relaxed state is maintained for 24 h, an equivalent amount of normal saline is injected into the expander capsule again to maintain expansion, and this operation is repeated two–three times. The relaxation training can effectively reduce the blood supply disorders occurring due to the tortuous and spasmodic blood vessels caused by the sudden decompression after removal of the expander in the second-stage surgery [18].
Related posts:
 Microcirculation Model for Invasive Animal Monitoring
Microcirculation Model for Invasive Animal Monitoring
 Composite Osseomusculocutaneous Thymus Allotransplantation Model
Composite Osseomusculocutaneous Thymus Allotransplantation Model
 In Vivo Chimera Model: Creation of Primary and Secondary Chimera
In Vivo Chimera Model: Creation of Primary and Secondary Chimera
 Experimental Model for Monitoring of Composite Tissue Transplantation Induced Trauma
Experimental Model for Monitoring of Composite Tissue Transplantation Induced Trauma
 Neuroma Model
Neuroma Model
 Defect Repairs After Resections of Laryngeal Cancer, Hypopharyngeal Cancer, and Cervical Esophageal Cancer
Defect Repairs After Resections of Laryngeal Cancer, Hypopharyngeal Cancer, and Cervical Esophageal Cancer
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


