Introduction
The skull base is traditionally divided into anterior, central, and posterior zones based principally on the appearance of the skull base as viewed from above (Fig. 2.1). This approach supports the general delineation of the intracranial compartment into the anterior, middle, and posterior fossae. The anterior skull base forms the broad floor of the anterior cranial fossa, which is filled predominantly with the frontal lobes of the brain. The anterior skull base is traditionally defined as the region of the skull base lying anterior to the lesser wing of sphenoid and planum sphenoidale (Fig. 2.2). The lesser wing of the sphenoid spans anterolaterally from the anterior clinoid process. The posterior and superior margins of the lesser wing form a curvilinear ridge that takes on the shape of a wing—hence its name. The lesser wing of the sphenoid bone fuses anteriorly with the posterior margin of the orbital plate of the frontal bone. The planum sphenoidale is the superomedial plate of sphenoid bone seen pos terior to the cribriform plate of ethmoid and anterior to the anterior wall of sella turcica (tuberculum sellae). Medially, the anterior skull base forms the roof of the nasal cavity and ethmoid sinus, including the cribriform plate of the ethmoid. Laterally, the orbital plates of the frontal bones form the orbital roof portion of the anterior skull base on either side. Posteriorly, the midline or parasagittal anterior skull base is constituted by the planum sphenoidale and laterally by the lesser wing of the sphenoid bone.1 The middle or central skull base is separated from the anterior skull base by a horizontal line along the anterior sellar margin extending laterally along the posterior margin of lesser wing of the sphenoid bone bilaterally, which includes the medial anterior clinoid processes.2
Midline or Parasagittal Anterior Skull Base Forming the Roof of the Nasal Cavity and Ethmoid Sinuses
The anterior skull base, especially in the region of the nasal vault and ethmoid roof, is only minimally ossified at birth and ossifies gradually from cartilage. The roof of the nasal cavity begins to ossify by around the age of 3 months and is predominantly ossified at 6 months. The crista galli, a midline triangleshaped, superiorly projecting bony process of the ethmoid bone, begins to ossify from the tip at 3 months and is usually ossified by the first year. The name is derived from the Latin and means crest of the cock (rooster’s comb). The crista galli provides attachment to the anteroinferior part of the falx cerebri and should not be confused with the frontal crest, a more anterior midline bony ridge–like portion of the frontal bones, which also provides attachment to the falx cerebri (Fig. 2.3). The crista galli is pneumatized in 10 to 15% of patients as identified on computed tomography (CT) scans. Although the crista galli is technically part of the ethmoid bone, pneumatization generally occurs as an extension of the left or right frontal sinus.3 The perpendicular plate of the ethmoid, which forms the superior portion of the bony nasal septum and is seen directly below the crista galli, begins to ossify at 6 months and fuses with the vomer, which forms the inferior portion of the bony nasal septum by around 2 years of age.1
The cribriform plate (lamina cribrosa) of the ethmoid in the adult is a horizontal perforated bony plate at the medial aspect of ethmoid bone, with deep grooves lying on either side of the midline crista galli. It forms part of the roof of the nasal cavity and constitutes the floor of the olfactory fossa lodging the olfactory bulbs (Fig. 2.4). The olfactory fossa is the lowest point in the anterior skull base. The perforations and foramina in the middle of the grooves are small and transmit the afferent olfactory nerve fibers from the nasal vault mucosa to the olfactory bulbs intracranially. The larger foramina at the medial aspect of the grooves transmit nerves to the superior nasal septum and those at the lateral aspect to the superior turbinate region. More than two-thirds of the population will have ossified posterior cribriform plates by 1 year of age, and most of the anterior skull base, including the cribriform plates, are ossified after 2 years; however, small gaps can be seen in the nasal roof until early in year 3 of life.
The ethmoid roof is formed by the vertically oriented lateral lamella of the cribriform plate of the ethmoid bone medially and the more horizontal fovea ethmoidalis of the orbital plate of frontal bone superolaterally. The vertical lateral lamella lies just lateral to the horizontal cribriform plate proper. The lateral lamella is 10 times thinner than the fovea ethmoidalis.4 The skull-base attachment of the middle turbinate of the nasal cavity to the anterior cribriform plate is quite delicate, and its detachment at surgery can damage the dura mater with resultant cerebrospinal fluid leak.
Ethmoid air cells lie inferior to the plane of cribriform plate until 3 months of age. By 6 months, they extend above the horizontal cribriform plate plane, and the more superolateral fovea ethmoidalis portion of ethmoid sinus roof begins to develop from the orbital plate of the frontal bone by 18 months and matures by 2 years of age. Knowledge of this lateral-to-medial slope of the anterior skull base is extremely important during transethmoidal surgical approaches to anterior skull-base lesions. Using the same axial plane of surgical dissection, which is safe along the more lateral ethmoid roof, could injure the brain and dura mater if extended medially to the region of cribriform plate.5
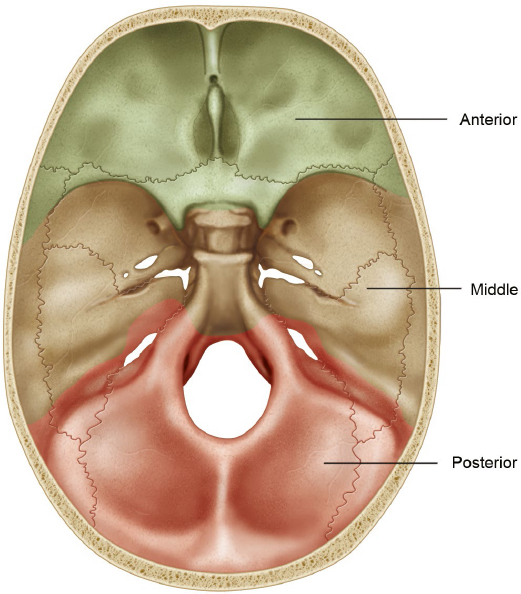
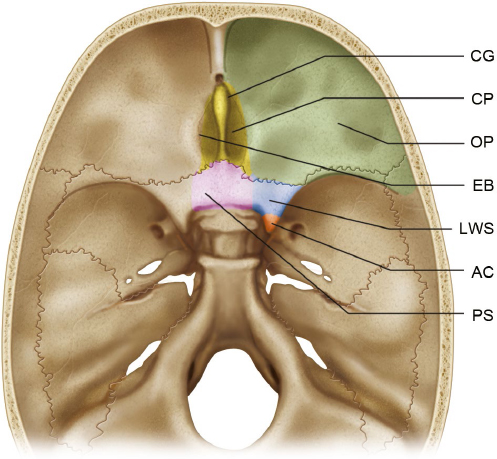
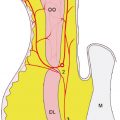
Fig. 2.2 Magnified view of the anterior skull base. The anterior clinoid process (AC) merges anteriorly with the lesser wing of the sphenoid bone (LWS). Medially, the lesser wing of the sphenoid merges with a flat portion of the sphenoid bone that serves as the ventral roof to the sphenoid sinus, the planum sphenoidale (PS). The lesser wing of the sphenoid is joined anteriorly with the orbital plate (OP) of the frontal bone. The orbital plate of the sphenoid bone serves as the roof of the orbit. The ethmoid bone (EB) is in the center of the anterior skull base and contains the cribriform plate (CP) and the crista galli (CG).
A horizontal line drawn along the roof of the ethmoid sinus passes through the orbit superior to the orbital vertical midpoint in most cases (88%), with 10% crossing at the midpoint and only 2% below that plane.6 Preoperative imaging should be critically reviewed to assess for a low-lying skull base. The safest anatomy is when the horizontal line drawn from the roof of the ethmoid crosses the upper third of the orbit; precautions to avoid injury to the skull base should be taken when the horizontal plane of the ethmoid roof crosses below the vertical midpoint of the orbit.1
The skull base also slopes downward in an anterior to posterior direction in the sagittal plane from the frontal recess to the planum sphenoidale along the ethmoid roof. The degree of slope is highly variable and should be assessed by preoperative imaging. During endoscopic sinus surgery, the skull base could be injured while using a front-to-back technique. Skull-base injury can be avoided by early identification using the back-to-front technique of endoscopic surgery whereby the skull base is easily located at the roof of sphenoid sinus after identifying the superior meatus and sphenoid ostium.7–11
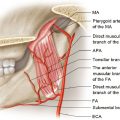
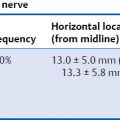
The Keros classification of the ethmoid roof and olfactory fossa into three types takes into account the vertical height of the lateral lamella of the ethmoid and the resultant depth of the olfactory fossa (Fig. 2.5). An olfactory fossa that is only 1 to 3 mm deep because of a nearly nonexistent lateral lamella constitutes a Keros type 1 (12%). The olfactory fossa is 4 to 7 mm deep in Keros type 2 (70%) and 8 to 16 mm deep in type 3 (18%) with progressively increasing vertical height of the lateral lamella.12 Asymmetry of more than 2 mm is seen in 8% of cases.13 During endoscopic surgery, Keros type 3 has the largest risk for iatrogenic injury to the lateral lamella. Also, the anterior ethmoidal artery could be iatrogenically injured in the anterior ethmoidal foramen (along with the anterior ethmoidal vein and nerve) (Fig. 2.6) lying between the ethmoid and frontal bones just anterolateral to the cribriform plate and cause catastrophic bleeding into the orbit. The posterior ethmoidal foramen containing the posterior ethmoidal artery, vein, and nerve lies between the ethmoid and sphenoid bones, just posterolateral to the cribriform plate of the ethmoid.
More Anterior Portions of Midline/Parasagittal Anterior Skull Base
The foramen cecum is a small midline pit lying between the frontal and ethmoid bones, just anterior to the crista galli of the ethmoid (Fig. 2.7). It is close to 4 mm in diameter at birth, and the ossification is usually complete by 2 years but can sometimes be delayed until the age of 5 years.14 Ossification defects in the region of the foramen cecum, nose, and forehead can lead to the formation of three subtypes of frontoethmoidal (sincipital) cephaloceles: frontonasal (40–60%), nasoethmoidal (30%), and nasoorbital (10%) cephaloceles. Associated ocular or intracranial abnormalities are present in 80% of cases with frontoethmoidal cephaloceles.15
During early intrauterine life, a small anterior skull base fontanel at the anterior boundary of the anterior skull base, called the fonticulus frontalis, lies between the superior partially ossified frontal bone and inferior nasal bones. At this time, there is also a small space filled with dura just posterior to the developing nasal bones and anterior to the cartilage of the developing nasal capsule, called the prenasal space. When the chondrocranium begins to ossify, the fonticulus frontalis closes, and failure of its closure leads to development of a frontonasal cephalocele. In this condition, a small portion of meninges with (meningoencephalocele) or without (meningocele) brain herniates into the forehead at the region of the glabella or dorsum of the nose through a patent fonticulus frontalis, between the frontal bone superiorly and the nasal bones inferiorly.16
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


