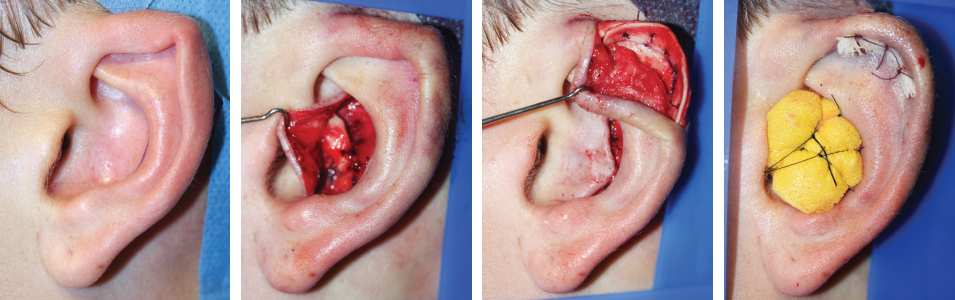
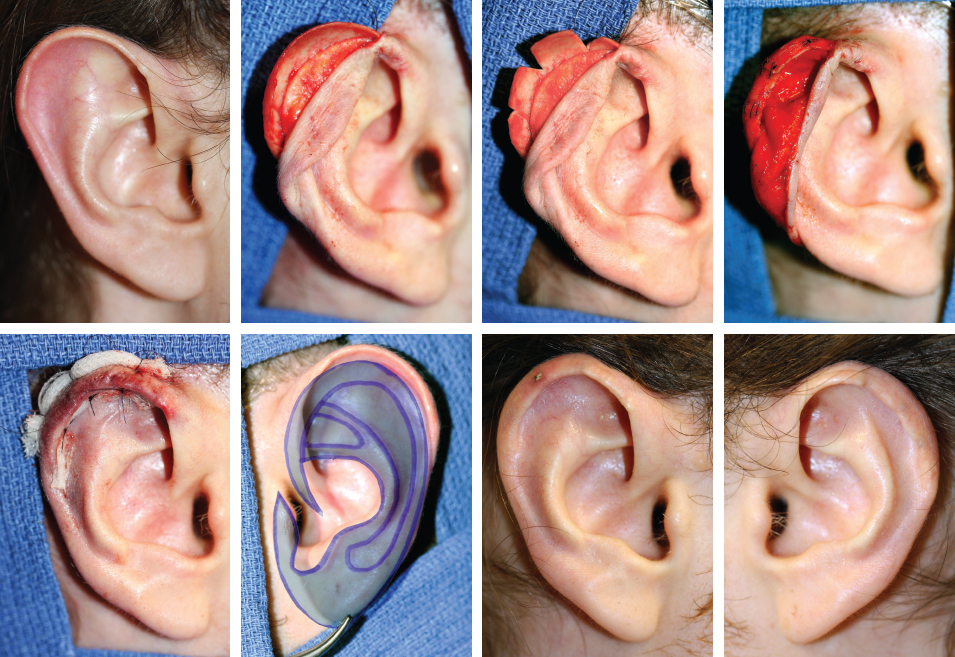
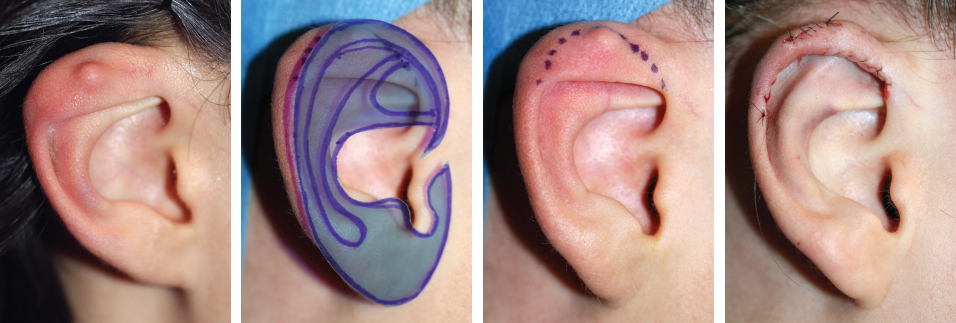
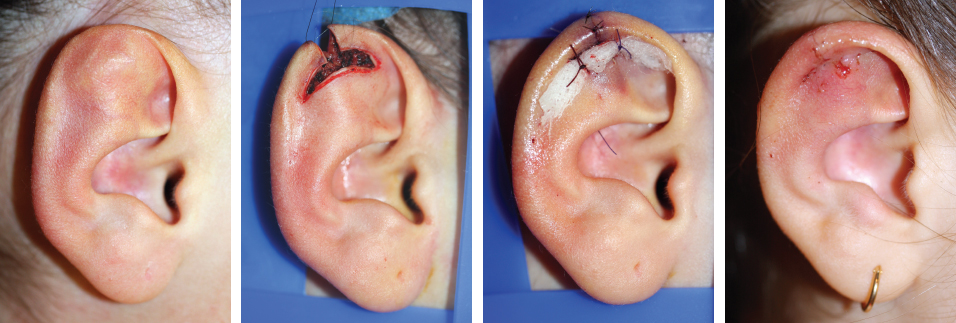
CHAPTER 14 Patients with an anomaly limited to the helical margin of the ear may often accept it as an aesthetic variation, because the ear is not smaller than the contralateral ear and can easily be hidden. Fig. 14-1 The shape of the helix on the right ear is abnormal, and the ear is a little smaller than the contralateral ear. The patient hides the upper part of her ears with long hair, yet the multiple piercings draw attention to the inferior part. The surgeon must correctly analyze the anomaly to determine the ideal size and shape of the ear before devising a reconstructive plan. An isolated anomaly of the helix can be simple to correct by a direct skin approach with remodeling of the fibrocartilaginous shape. Other cases may require the addition of a cartilage graft to re-create the delicate curvature of the helix. Fig. 14-2 A template of the contralateral ear confirms that the size of the anomalous ear is similar. A direct approach and reduction of the free edge of the helical fibrocartilage were performed, and the small skin irregularity located on the helix was excised. Fig. 14-3 In this case a small part of the upper helix is unfolded, with an adjacent scaphoid fossa convexity. A small transfixion excision of the helix and elliptical excision of the adjacent fibrocartilage corrected this small anomaly. This ear was pointed because of the shape of the helix, which could not be corrected by simply reshaping. To obtain a round margin, a conchal graft was taken on the same side through an anterior approach. A second posterior skin approach to the helix allowed exposure of the anomaly and correct fixation of the reshaped conchal graft, reproducing the harmonious curvature of the helix. Bolster sutures helped to adapt the skin to the conchal graft and were removed on day 4. Fig. 14-5 This is a unilateral abnormal-shaped helix. To make a round ear shape, the surgeon must see that the adjacent scapha is narrow. A conchal graft harvested on the same side will correct the small anomaly. An unfolded helix is a frequent anomaly, often occurring bilaterally. When it is unilateral, the surgeon must consider that folding the helix will reduce the overall size of the operated ear. Fig. 14-6 A unilateral unfolded helix is seen. The ear is slightly larger than the contralateral ear, when compared with the template. A posterior skin approach was used to expose the helix. Small triangles of fibrocartilage were excised from the free edge of the helix. Closure of the defects allowed the helix to be “rolled in.” This technique created a slight reduction in the overall size of the ear. The sharp anterior edge of the helix must be perfectly adapted, because it is easy to create visible irregularities and notching with this procedure.
Anomalies of the Upper Part
of the Ear
HELIX

Abnormal Shape

Unfolded Helix

Plastic Surgery Key
Fastest Plastic Surgery & Dermatology Insight Engine