Ankle and Foot Bone Tumors
Robert J. Steffner
Raffi S. Avedian
Sahitya K. Denduluri
DEFINITION
Bone tumors of the foot and ankle are usually primary tumors. Metastatic bone cancer to sites below the knee is rare but not impossible.
Primary bone tumors can be benign, low-grade malignant, or high-grade malignant.
Surgery is considered for benign tumors with progressive growth or those producing symptoms. Malignant bone tumors are generally operative in both a curative and palliative setting.
ANATOMY
There is minimal soft tissue coverage in the ankle and foot. Surgical resections requiring skin excision and/or placement of bulk cortical allograft should consider the need for soft tissue coverage to minimize the risk of infection and nonunion.
When functional deficit and donor site morbidity for free tissue transfer are anticipated, consideration should be given to below-knee amputation. Patients may recover faster and have better long-term function with a prosthesis.1
PATIENT HISTORY AND PHYSICAL FINDINGS
It is important to ask patients about prior trauma and infections at the site of concern.
A clinical history focusing on the duration of symptoms, presence of night pain, and systemic symptoms can help delineate benign from malignant etiologies.
Physical exam focuses on the presence of prior incisions, skin mobility over the tumor, and neurovascular status distal to the site of tumor involvement.
IMAGING
Obtain plain radiographs of the involved site.
Perform an MRI scan with and without contrast to assess the extent of tumor and involvement of critical structures such as tendons, nerves, and vessels. Also perform a whole bone MRI to demonstrate the extent of intramedullary involvement of tumor and look for skip lesions.
Make every effort to obtain any prior imaging for comparison.
Quality of imaging and the interpretation of imaging are vital for surgical planning.
Upon diagnosis of a primary bone malignancy, staging studies are performed to assess for regional or distant metastatic disease. This generally requires a chest CT and whole body bone scan.
DIFFERENTIAL DIAGNOSIS
Benign and malignant bone tumors can be found in the foot and ankle. Distinguishing between benign and malignant guides the extent of surgical management.
Benign tumors include simple cyst, intraosseous ganglion, and enchondroma.
Benign but active tumors include aneurysmal bone cyst (primary or secondary), giant cell tumor, osteoid osteoma, and, in pediatric patients, chondroblastoma.
Malignant bone tumors include osteosarcoma, chondrosarcoma, Ewing sarcoma, primary lymphoma of bone, and metastatic carcinoma.
NONOPERATIVE MANAGEMENT
Benign-appearing lesions that are not causing symptoms can be followed with serial imaging. Stable appearance on serial imaging studies supports nonsurgical management.
SURGICAL MANAGEMENT
Symptomatic benign bone tumors and benign but active bone tumors are most often treated with intralesional curettage or marginal excision.
Malignant bone tumors may require multidisciplinary management with the possible need for chemotherapy and/or radiation in addition to surgery.
In nonmetastatic or oligometastatic primary bone cancer, the goal of surgery is resection with negative margins.
Preoperative Planning
If needed, size-matched fresh-frozen allografts should be coordinated from an appropriate vendor well ahead of time. The surgeon should assure that the graft has been delivered to the hospital. It is wise to have a back-up allograft available.
Bone cuts are planned off T1-sequences from the first MRI scan. It is important to appreciate any soft tissue extensions and to look for fat planes around neurovascular structures to make sure they are free from tumor. Determination of appropriate margins is based on the specific diagnosis and the type of tissue at the level of resection.
Approach
An oncologic approach allows for a limited tissue biopsy while maintaining the possibility of wide resection in the setting of a malignant diagnosis. If oncologic principles are followed, the majority of patients will be eligible for limb salvage.2
TECHNIQUES
▪ Benign Bone Tumor of the Talus (TECH FIG 1A,B)
Patient positioned supine with an ipsilateral hip bump on a radiolucent table
Tourniquet used after gravity exsanguination
Localize tumor with intraoperative fluoroscopy
To access talar body, an oblique osteotomy of the medial malleolus or distal fibula is often required. The surgeon may predrill bone in a lag-by-technique fashion before the osteotomy. This facilitates repair at the end of the surgery.
A cortical window or cartilage flap is created with a curette or high-speed bur to access the bone tumor (TECH FIG 1C).
Tissue is removed and sent for frozen section. If the pathology report is consistent with a benign tumor and matches the patient’s clinical history and imaging, the surgery proceeds.
The cortical window is expanded to adequately visualize and remove the tumor through intralesional curettage.
Tumor margins are extended with use of a high-speed bur to smooth out the internal cavity of the cyst. Adjuvant treatments such as cryosurgery (liquid nitrogen) and argon beam coagulation can penetrate bone and further the zone of tumor kill. These measures lower the risk of local tumor recurrence.3
Care should be taken near cartilage and growth plates to avoid damage to these structures. It is appropriate to accept a higher risk of local tumor recurrence in order to avoid injury to these structures.
The resultant bone defect is filled with a substance of the surgeon’s choice. In general, we use allograft in young patients; artificial bone void filler in young adults (mixture of calcium phosphate and calcium sulfate) and cement in older individuals.
Supplementary internal fixation may be needed in weight-bearing locations and large defects (TECH FIG 1D).
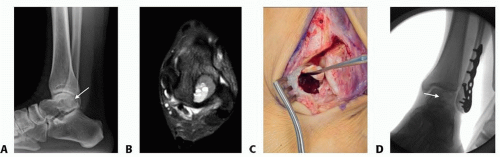 TECH FIG 1 • A. Lateral radiograph of a secondary Aneurysmal Bone Cyst of the talar body (arrow). B. Axial Fat-suppressed T2 MRI image demonstrating fluid-fluid levels. C. Photo after oblique osteotomy of the distal fibula to access the talar body. A cartilage flap is made to access the bone tumor. D. Fluoroscopic image demonstrating cancellous allograft filler in the talar body and internal fixation of the distal fibular osteotomy (arrow). |
▪ Malignant Bone Tumors of the Foot and Ankle
General Principles
Use separate instruments for tumor resection and bone defect reconstruction.
Obtain a thorough preoperative neurovascular exam.
Consider an epidural catheter that can be test-dosed before surgery and used once a postoperative nerve exam is obtained.
Use a thigh tourniquet and gravity to exsanguinate the leg.
Hold paralytic medications if a nerve dissection is needed.
Ellipse biopsy tract and keep in continuity with the resected tumor.
Generally work from normal anatomy to abnormal anatomy.
Clip or tie any arteries or veins that could be used for microvascular anastomosis.
Measure bone cuts several times before cutting.
After the bone cut, send a marrow margin for frozen section from the nonresection side.
Orient resected specimens before sending to pathology.
Fresh-frozen allografts are opened when frozen sections are negative. The allograft should be cultured and then placed in warm water bath with antibiotics for thirty minutes before use.
Distal Fibula Resection
Lateral position on a beanbag. Straight lateral incision (TECH FIG 2A).
Anteriorly, assess relationship of tumor with extensor digitorium longus and peroneus tertius.
Posteriorly, assess relationship of tumor with peroneus longus and brevis and flexor hallucis longus (FHL).
At the ankle joint, release the tibiofibular ligaments, talofibular ligaments, and calcaneofibular ligament.Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree