Alopecia
Scott Walter
Mary Barrett
Lynne J. Goldberg
Nonscarring Alopecia
ANDROGENETIC ALOPECIA
Definition and Epidemiology
Androgenetic alopecia (AGA), which is the most common alopecia in adults, can occur in children and adolescents. It is characterized not by a true loss of hair, but by a slow and progressive miniaturization of the hair follicle, with an increase in the telogen to anagen hair ratio.1 This leads to an apparent thinning of the hair in characteristic patterns on the scalp. Both a genetic predisposition and androgen hormones play a role in the pathogenesis of AGA.1,2
The exact incidence and prevalence of AGA in children is not well established. One study of nearly 500 15- to 17-year-old males found that 15.5% had some degree of AGA.3 For most children, onset is typically after puberty, but can occur in prepubertal children as young as 6.4 The average age of onset in children ranges from 13.5 to 15 years old.4,5 Two larger studies in adolescents showed a male predominance, with male to female ratio ranging from 2:1 to 4.3:1, which is similar to the adult population.5,6 Other studies have shown a slight female predominance in children.4,7 A strong family history of alopecia is common in children with AGA, present in 72.1% to 83% of affected patients, which is greater than that reported for adults (30% to 64.5%).5,6 In a series of 20 prepubertal children with AGA, all had a strong family history—with 9 patients having one parent affected and 11 having both parents affected.4 Some other dermatologic disorders have been associated with AGA, including seborrheic dermatitis, acne vulgaris, and atopic dermatitis.6 Severe acne and hirsutism in females is associated with a more severe AGA presentation.1
Etiology
As the name suggests, AGA is both androgen-dependent and genetically inherited. Males castrated before puberty do not develop AGA, which supports the role of androgens.8 However, the exact mechanism of pathogenesis is not well understood—especially in the pediatric population.
Miniaturization occurs when androgen hormones act directly upon terminal follicles, converting them to vellus-like follicles. As they miniaturize, the hair cycle shortens, leading to increasingly smaller and more superficial follicles with shorter, thinner, and paler hair shafts. Shortening of the anagen phase results in a greater number of overall hairs in the telogen phase.1 Certain follicles on the scalp have been found to be more susceptible to the effects of excess androgens, which leads to the characteristic male and female patterns of hair loss—in males on the vertex and frontotemporal scalp and on the crown in females.1 Androgen receptors and type II 5-α reductase, the enzyme that converts testosterone to the active metabolite dihydrotestosterone, are found in higher levels in the outer root sheath and dermal papillae of follicles in these areas.9,10 The relationship between blood levels of androgen hormones in the development of AGA is controversial, with studies in children and adolescents yielding conflicting results. Nevertheless, hyperandrogenemia has been detected in association with some cases of pediatric AGA, including
in patients with polycystic ovarian syndrome and late-onset congenital adrenal hyperplasia.4,5,6,11,12
in patients with polycystic ovarian syndrome and late-onset congenital adrenal hyperplasia.4,5,6,11,12
Studies in children with AGA consistently show a family history of patterned hair loss, and concordance rates in monozygotic twins range from 80% to 90%, suggesting a strong genetic predisposition.2,4,6 Although the exact genetic inheritance is not known, it is most likely polygenic.13,14,15 In adults, polymorphisms in the 5-alpha-reductase enzyme and androgen receptor have been found to be associated with AGA, and mutations in 17-α-hydroxylase are associated with premature AGA.14,15,16
Clinical Presentation
AGA presents with gradual onset hair thinning localized to the androgen-dependent parts of the scalp. Hair in affected areas is thinner, shorter, and finer, leading to classic patterns of loss as described originally by Hamilton and Ludwig.17,18 The majority of adult men have loss localized to the vertex and recession in the frontotemporal region, whereas adult females typically preserve their frontal hairline with loss more prominent on the crown of the scalp. The patterns of hair loss in children with AGA vary, and usually present more mildly compared with adults.19 Prepubertal males may present with classically female pattern, and sometimes show frontal prominence.4,5 This is characterized by a widened central part (Figure 16-1). Onset in adolescents usually presents in classic gender-specific patterns.6 The occiput is usually spared in all patients. Diagnosis in children is supported by trichoscopy showing greater than 20% hair diameter diversity (miniaturization).4
 FIGURE 16-1. Male pattern hair loss in a 17-year-old boy. Note the bitemporal recession of the hair line and the thinning of hair on the crown. |
Histologic Findings
The major histopathologic finding in AGA is miniaturization of hair follicles with a subsequent decrease in the terminal:vellus (T:V) size ratio (Figure 16-2). The normal T:V ratio is approximately 6-8:1,20 but a ratio of 4:1 or less is considered compatible with AGA,21 and a ratio of 2:1 or less is common. Additional findings include a normal overall number of follicles, a slight increase in the percentage of follicles in catagen or telogen phase (up to 20%), and the presence of follicular stelae (fibrous tracts or streamers) underlying the miniaturized hairs.22 In a small study of biopsies of pediatric AGA, 57% showed varying degrees of a lymphocytic perifollicular inflammation and accompanying fibrosis.5 However, inflammation is not a consistent feature, and peribulbar inflammation or associated follicular destruction should be absent. Scarring may occur in longstanding AGA,22 but is unlikely in the pediatric population.
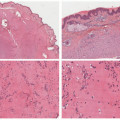
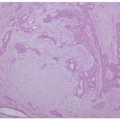
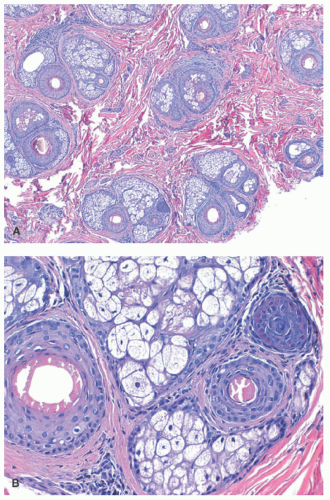 FIGURE 16-2. Histopathology of androgenetic alopecia in a 16-year-old girl. A, Low-power view of the isthmus reveals a mixture of terminal and vellus hair follicles with a terminal to vellus ratio of approximately 1:1 (H&E, ×4). B, Higher power of a follicular unit with one terminal and two vellus hair follicles (H&E, ×20). |
Differential Diagnosis
The clinical differential diagnosis of AGA includes alopecia areata (AA) and telogen effluvium (TE). In most cases, these can be distinguished by the pattern of hair loss, with AA typically leading to patchy hair loss in well-demarcated areas, and TE causing more global hair thinning. Diffuse AA lacks the typical patchy distribution of the classic type and may pose a diagnostic challenge.
Histologically, AA shares some common features with AGA, but typically shows a much more marked shift away from anagen, with catagen/telogen counts from 50% to 100%. Additionally, peribulbar lymphocytic inflammation is often present,23 along with dilated follicular infundibula, trichomalacia, and small follicles with abnormal morphology lacking a central hair shaft.
TE in its acute form displays a normal total number of follicles with an increased proportion in catagen and telogen phases (not exceeding 50%), and fibrous stelae underlying these follicles. Chronic TE can have a variable percentage of catagen/telogen follicles and may closely mimic a normal scalp biopsy. Neither acute nor chronic TE displays the miniaturization of follicles characteristic of AGA.
CAPSULE SUMMARY
ANDROGENETIC ALOPECIA
AGA is an uncommon cause of alopecia in children. It is caused by the action of androgen hormones on scalp hair follicles, leading to miniaturization and the appearance of hair loss. It is polygenic in inheritance, and presents as a gradual thinning of hair at the vertex and frontotemporal regions of the scalp in males or on the crown of the scalp in females and prepubertal children. Histopathologic findings include miniaturization of hair follicles with an associated decrease in the T:V size ratio and a mild increase in the number of catagen/telogen follicles.
TELOGEN EFFLUVIUM
Definition and Epidemiology
TE is a nonscarring, diffuse alopecia characterized by a disproportionate loss of telogen hairs after a trigger that disrupts the normal hair cycle.24,25
The exact prevalence and incidence of TE is not known in adults or children, but is likely similar in the two groups.26 It is one of the most common causes of nonscarring hair loss in children, accounting for 10% to 17.6% all forms of alopecia in one case series.5,27,28 The mean age at presentation has been reported as 8 years, with females being more commonly affected.28
Etiology
Normally, hair follicles cycle asynchronously, with about 10% in telogen phase at any given time.29 This leads to a normal daily physiologic hair shedding of 100 to 200 hairs. In TE, a trigger causes a synchrony of the hair cycle, such that a large number of follicles shift together from anagen to telogen phase, resulting in marked hair shedding 2 to 3 months after the trigger.26
Potential triggers include psychologic or physiologic stress, or hormonal changes. The most common causes in children are high-grade fever, frequent illness, and iron deficiency anemia.28 Other causes may include surgery, medications, other nutritional deficiency (zinc, protein, essential fatty acids), endocrine disorders, and immunizations.30,31,32,33 No trigger is identified in about one-third of cases. Commonly used medications in the pediatric population that may trigger TE include psychotropics (lithium and antidepressants), systemic retinoids, anticonvulsants, and oral contraceptives.24,34 The exact mechanism behind how these triggers lead to TE is not well understood.
Clinical Presentation
Patients with TE present with an acute and diffuse decrease in density of hair, typically with a loss of less than 50% of the hair.35 Onset occurs approximately 2 to 3 months after the triggering event, is reversible, and lasts a total of 6 months.24 Shedding that persists longer than 6 months is classified as chronic TE,35 which is typically seen in middle-aged women, but has been reported in children experiencing chronic starvation.36 Distribution of hair loss is usually diffuse, but may be more noticeable in the bitemporal area in some patients.35 Although trichoscopic findings are nonspecific, they may provide clues to the diagnosis and include empty follicles, lack of variability in diameter, brown perifollicular discoloration, and short, upright regrowing hairs during the regrowth phase.37,38,39
Histologic Findings
A biopsy of TE may show very subtle findings, as the total number of hair follicles is normal. Acute cases often show a shift toward catagen and telogen phases (generally greater than 20%), although a lower percentage does not exclude the diagnosis.31 Chronic TE may have a normal percentage of follicles in catagen/telogen phases because of the waxing and waning nature of the disease.40 Biopsies with an increase in catagen/telogen follicles show normal counts superficially at the level of the isthmus, with decreased numbers of follicles and fibrous stelae at deeper levels. Importantly, neither acute nor chronic TE features loss or miniaturization of follicles or significant inflammation.41
Differential Diagnosis
The clinical differential diagnosis of TE includes AGA and AA. AGA tends to follow a slower course without regrowth. AA has a similarly abrupt onset, but tends to lead to patchy hair loss. Diffuse AA may be difficult to differentiate from TE on a clinical basis.
The histopathologic differential diagnosis of TE is quite broad, as a variety of etiologies can result in an increased percentage of catagen/telogen-phase follicles. These include AGA, AA, traction alopecia, trichotillomania, and psoriatic alopecia. Accurate diagnosis often depends on the presence of a characteristic clinical history.
AGA may show an increase in catagen/telogen follicles, but a more conspicuous finding is miniaturization of follicles. Similarly, AA displays prominent miniaturization, as well as findings such as peribulbar lymphocytic inflammation, trichomalacia, a lack of hair shaft production in miniaturized follicles, and dilation and keratotic plugging of follicular infundibula. Traction alopecia may show normal follicular size and number in addition to a mildly elevated catagen/telogen count, but there is often follicular dropout, and the presence of trichomalacia, pigment casts within follicles, and sebaceous glands that lack associated follicles may help distinguish it from TE. Trichotillomania shows features similar to those of traction alopecia, with the addition of disrupted and deformed follicles. Finally, psoriatic alopecia often has a markedly increased catagen/telogen count, but overlying changes of psoriasis are also seen.
CAPSULE SUMMARY
TELOGEN EFFLUVIUM
TE is a diffuse, nonscarring alopecia that is relatively common in children. It is often triggered by an illness or a medication and presents with acute diffuse hair loss. It begins 2 to 3 months after the trigger and lasts approximately 6 months. The pathophysiology involves a large number of follicles simultaneously undergoing premature or prolonged shift from the anagen growth phase to catagen and telogen phases. Histologically, it displays a normal number of follicles with a shift from anagen to catagen and telogen phases, but findings may be subtle or absent. It is a histopathologic diagnosis of exclusion, best made when there is a characteristic clinical history combined with a lack of additional findings such as miniaturization, trichomalacia, or inflammation.
ALOPECIA AREATA
Definition and Epidemiology
AA is the most common type of alopecia seen in children and is characterized by an acute onset, nonscarring alopecia of the scalp or any hair-bearing area.5,42 It is classified as a polygenic, lymphocyte-mediated autoimmune disease specific to the hair follicle.
The estimated prevalence is 0.1% to 0.2% in the general population, with 20% of cases occurring in the pediatric population.43,44 Although there is no gender ratio difference in adults, studies in children favor a slight female predominance, with a female to male ratio ranging from 1.6 to 2.5:1.43,45,46 There is no racial predilection.46 The mean age of onset in children ranges from 4.2 to 5.7, with onset peaking between ages 2 and 6.43,45 AA is rare in infancy, but has been reported.43 A total of 10% to 19% of patients have a positive family history of AA.45,47,48,49
Etiology
AA is a lymphocyte-mediated, genetically influenced autoimmune disease restricted to the hair follicle.50,51 It is likely polygenic in nature, with numerous genes identified that are involved with both the innate and acquired immune system. Genes encoding cytotoxic T-lymphocyte-associated antigen 4, regulatory T cells, interleukin-2, and human leukocyte antigen class II have all been implicated.52 There is a positive family history in 4% to 28% of patients with AA, and 55% concordance in monozygotic twins.53,54
Hair loss in AA is mediated by CD8+ T-lymphocytes activated by disruption of the immune privilege inherent to the hair follicle.55,56 T cells found in the peribulbar infiltrate induce keratinocyte apoptosis, leading to aberration in the follicle growth cycle.51,57 The degree of inflammation determines whether the hair follicle remains in anagen or converts to telogen phase, with more inflammation leading to the latter.50,51
AA is commonly seen in association with other inflammatory and autoimmune disorders. Atopic dermatitis is the most commonly associated disorder in children, with prevalence ranging from 28% to 61% among children with AA. It is associated with more severe alopecia.45,58 Other associated disorders include thyroid disease, Down syndrome, vitiligo, juvenile idiopathic arthritis, psoriasis, and other autoimmune diseases.45,58 A recent study in children found that an increased incidence of thyroid disease was seen in AA patients with concomitant atopy, Down syndrome, or a family history of thyroid disease.58
Environmental factors such as stress, hormones, and infectious agents have been linked to the development of AA, although clear etiologic evidence is lacking.50
Clinical Presentation
AA presents acutely with asymptomatic patches of hair loss on any hair-bearing area. It affects the scalp in the majority of patients and typically appears as well-defined, focal patches of alopecia without epidermal change (Figure 16-3).46 AA can be classified either on the basis of pattern of hair loss or severity. Patterns include patchy alopecia with partial loss, typically on the scalp; alopecia totalis (AT) defined by a complete loss of scalp hair; and alopecia universalis (AU)
with complete loss of scalp and body hair. The ophiasis pattern presents with band-like, circumferential loss of hair across the temporal, parietal, and occipital scalp. Severity is classified by an overall percentage of hair loss: mild (<25%), moderate (26% to 50%), or extensive (>50%).59 The reported prevalence of severe disease in affected children of different populations ranges from 13% to 66%.43,47,48,49,58,60,61 Early age of onset is associated with more severe disease,60,62 and 5% of all AA cases may progress to AT/AU.63
with complete loss of scalp and body hair. The ophiasis pattern presents with band-like, circumferential loss of hair across the temporal, parietal, and occipital scalp. Severity is classified by an overall percentage of hair loss: mild (<25%), moderate (26% to 50%), or extensive (>50%).59 The reported prevalence of severe disease in affected children of different populations ranges from 13% to 66%.43,47,48,49,58,60,61 Early age of onset is associated with more severe disease,60,62 and 5% of all AA cases may progress to AT/AU.63
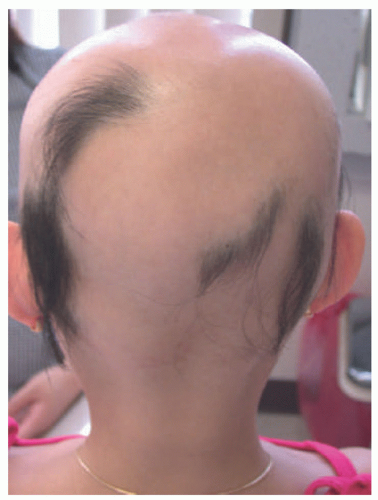 FIGURE 16-3. Alopecia areata in a 6-year-old girl. Extensive, patchy, nonscarring hair loss. |
The characteristic lesions of AA are well-defined, round, or oval patches of complete hair loss with underlying normal skin tone. Patches occasionally have a slight red or orange-pink hue.50 Closer examination often reveals “exclamation point” hairs, which represent short, proximally tapered hairs most often seen at the border or within the patch.46 The other trichoscopic features of AA include black dots (44%-70% of patients), yellow dots (63%-94%), broken hairs (45%-58%), and vellus hairs (33%-72%).37 Black dots represent fractured hair shafts in active disease, whereas yellow dots are enlarged follicular infundibula containing keratinous and sebaceous material, indicating inactive, late-stage, or severe disease.37,51,64 Early regrowth of hair is often non- or hypopigmented.65 Hairs at the periphery of active disease patches may be extracted with minimal force and no pain, indicating a positive hair-pull test.66
Nail changes are seen in AA in 26.5% to 40% of children, with pitting being the most common change observed.43,48,49,51,67,68 Others include onychorrhexis (longitudinal splitting of the plate), Beau lines (horizontal grooves), onychomadesis (shedding at the proximal end), trachyonychia (rough, longitudinally ridged nails), koilonychia (spoon-shaped nails), leukonychia (white macules), and red-spotted lunulae.66 Nail disease is associated with a more severe disease in children.43,48,49
Histologic Findings
The pathologic changes in AA depend on the stage of disease. In early (acute or subacute) disease, hair counts are normal, but there is a shift to catagen and telogen phases.41,69 Over time, there is a marked decrease in follicular size (Figure 16-4). An infiltrate of lymphocytes around follicular bulbs is a classic, albeit inconsistent finding (Figure 16-4).23 Other diagnostic features are the presence of follicles that either produce minute or no hair shafts, deformed or distorted hair shafts (trichomalacia), lymphocytic exocytosis into follicular epithelium, pigment casts (fragments of displaced pigmented matrix or cortical cells),41 and dilated follicular infundibula plugged with keratin.23
Chronic AA also typically has a normal or near-normal number of follicles,69 with most or all follicles being miniaturized, and a marked shift approaching 100% to catagen and telogen phases. Peribulbar inflammation may be sparse or absent in chronic disease.41 If AA persists for many years, permanent follicular loss may occur.70
Differential Diagnosis
AGA also features follicle miniaturization, but has a more modest shift to catagen and telogen phases, and does not feature peribulbar inflammation, trichomalacia, or dilated follicular infundibula. Psoriatic alopecia typically has accompanying changes of psoriasis and sebaceous gland atrophy.69 Trichotillomania can also have a shift into catagen/telogen phases, trichomalacia, and pigment casts, but these may be less pronounced, and miniaturization is absent. Syphilitic alopecia can closely mimic AA, featuring extensive miniaturization of follicles, a marked shift to catagen/telogen counts approaching 100%, and a peribulbar infiltrate of lymphocytes with an occasional extension of the inflammation up the follicle to the isthmus. However, syphilis is more likely to have plasma cells in the inflammatory infiltrate than AA.71,72,73
CAPSULE SUMMARY
ALOPECIA AREATA
AA is the most common cause of hair loss in children. It is acute in onset and may present with discrete round patches of hair loss, band-like loss, diffuse loss, or a total loss of all scalp or body hair. Histologically, AA features miniaturization of follicles and an increase in catagen/telogen hairs, with both changes becoming more marked as the disease progresses. Peribulbar lymphocytic inflammation is a characteristic finding, but is not always present. Although AA does not cause scarring, longstanding disease may progress to follicular dropout and permanent hair loss.
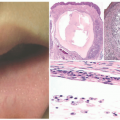
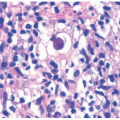
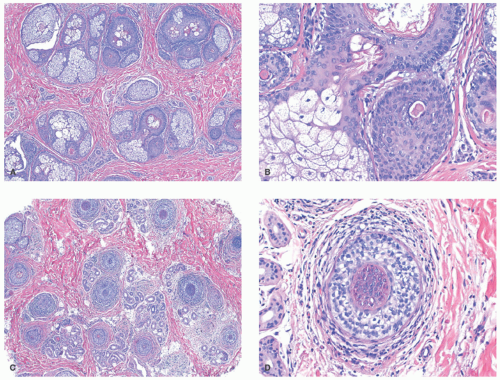 FIGURE 16-4. Histopathology of alopecia areata in an 18-year-old boy. A, Low-power view of the isthmus showing the absence of terminal hair shafts (H&E, ×4). B, High-power view of follicles with absent hair shafts typical of alopecia areata (H&E, ×20). (C) Low- and (D) high-power view at the suprabulbar level showing marked perifollicular inflammation (H&E, ×4; H&E, ×20). |
TRICHOTILLOMANIA
Definition and Epidemiology
Trichotillomania (TTM) is a self-induced form of traction alopecia caused by habitual plucking, pulling, or twisting of hairs, that is classified as an obsessive compulsive disorder.
The prevalence of TTM in children with alopecia ranges from 2% to 9.8%,5,28,74 with an estimated lifetime prevalence of 0.6% to 4.0%.75 In young children, males and females tend to be effected equally, with female predominance increasing with age.76,77,78 Peak onset occurs between 9 and 13 years, but has been reported in children as young as 1.78,79,80,81 Later age of onset is associated with increased severity, less responsiveness to treatment, and a higher likelihood of psychiatric comorbidities.76,80 About 5% to 8% of patients endorse a family history of TTM.82
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


