Alopecia (hair loss) is one of the ten most common causes of skin-related visits to physicians in the United States. Alopecia can be classified as scarring or nonscarring, and, although this is an important categorization, it is important to note that some alopecia can be both nonscarring and scarring, depending on the clinical circumstances (e.g., tinea capitis with kerion formation).
Nonscarring Alopecia
- •
Alopecia areata
- •
Anagen effluvium
- •
Androgenetic alopecia
- •
Syphilitic alopecia
- •
Telogen effluvium
- •
Tinea capitis (rarely scarring)
- •
Traction alopecia (can scar)
Scarring Alopecia
- •
Central centrifugal scarring alopecia
- •
Discoid lupus erythematosus
- •
Folliculitis decalvans
- •
Frontal fibrosing alopecia
Important History Questions
When did you first notice that you were losing hair?
Sudden diffuse hair loss favors telogen effluvium, anagen effluvium, or diffuse alopecia areata, whereas most other types of alopecia are insidious in onset (e.g., androgenic alopecia).
What products do you put on your hair?
Harsh chemicals that straighten hair (relaxers) or curl hair (perms) can damage it, yielding an alopecia.
Do you have any other known medical conditions?
Lupus erythematosus, secondary syphilis, thyroid disease, or chronic anemia may be associated with alopecia.
Have there been recent changes in your health?
A recent and significant physical stressor (e.g., pregnancy, marked weight loss, sustained high fever, major surgery, significant blood loss) can induce telogen effluvium.
What medications are you taking, and are any of these new?
Some medications can occasionally cause telogen effluvium (e.g., anticoagulants, oral retinoids, beta blockers, lithium), or anagen effluvium (e.g., chemotherapeutic agents).
Do you find yourself pulling on your hair under stress?
Trichotillomania is an alopecia caused by mechanical pulling of the hair. Some patients will openly admit to pulling at their hair, whereas others will hide such behavior.
Important Physical Findings
What is the distribution of hair loss?
The distribution of hair loss is important because it may be discrete (e.g., alopecia areata), patchy (syphilitic so-called moth-eaten alopecia), patterned (e.g., male-female pattern alopecia), or diffuse (e.g., telogen effluvium).
Is there evidence of inflammation or pustules?
Pustules may be indicative of folliculitis decalvans, dissecting cellulitis, or dermatophyte infection.
Is there evidence of epidermal changes in addition to the alopecia?
Epidermal changes, such as scale and crusting, may be seen in discoid lupus erythematosus or lichen planus, whereas many other forms of alopecia, such as alopecia areata, manifest little epidermal pathology.
Is there any scarring?
Alopecia may be divided into scarring (e.g., lupus erythematosus) and nonscarring forms (e.g., alopecia areata), so the presence of scar is significant. Some alopecias may be scarring or nonscarring (e.g., tinea capitis).
Is there hair loss in other hairy areas?
Involved eyebrows or eyelashes may favor trichotillomania, alopecia areata, or syphilitic alopecia.
Are there nail changes?
Beau lines may suggest telogen effluvium, whereas rough nails may suggest alopecia areata, and the formation of pterygium (e.g., split nails, often with a triangular lunula) may favor lichen planus.
Androgenic Alopecia
ICD10 codes L64.9
GENETIC DISORDER
Pathogenesis
Androgenic (androgenetic) alopecia is the most common cause of hair loss in men and women. By age 50 years, about 50% of men will demonstrate significant androgenic alopecia and, at age 60 years, 50% of women will demonstrate this same condition. There is a definitive genetic component, with mutations in the androgen receptor gene playing a role. Androgenic alopecia is a result of increased follicular activity of 5α-reductase in men and increased dehydrogenase enzyme levels in women. In women, other mechanisms may also be important; thus, some authorities prefer the term female pattern hair loss. The increased enzymatic activity causes a short anagen (growing) stage in hair follicles, resulting in small, nonpigmented (miniaturized) hairs that are barely visible.
Clinical Features
- •
Women demonstrate a pattern of diffuse thinning on the vertex scalp, with general preservation of the front hairline.
- •
Although female pattern hair loss is most noticeable around the time of menopause, the thinning develops earlier in some women ( Fig. 24.1 ).

Fig. 24.1
Typical diffuse pattern of hair loss on the vertex of the scalp in a woman.
- •
Men demonstrate recession of the bilateral temporal hairline, with or without thinning of the crown ( Figs. 24.2–24.4 ).

Fig. 24.2
Moderately severe thinning of the frontoparietal area and crown in a man.
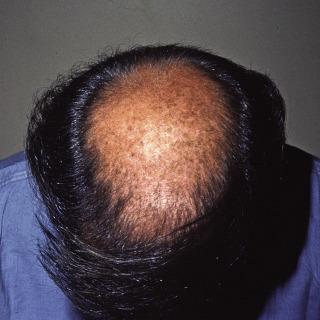
Fig. 24.3
Severe androgenic alopecia of the crown in a man.

Fig. 24.4
Almost complete loss of hair in the frontoparietal area and crown in a man. Note the scar from excision of a skin cancer.
- •
Severe cases in men demonstrate only a residual rim of hair around the posterior hairline.
Diagnosis
- •
The clinical presentation is usually diagnostic, but early-onset androgenic alopecia, which can occur as early as adolescence, can be difficult to diagnose and difficult for the patient to accept.
- •
Biopsy (with a 4-mm or larger punch) may not be diagnostic for only androgenic alopecia, but it can exclude a scarring and/or inflammatory alopecia. Miniaturization of hairs and increased sebaceous gland activity is compatible with androgenic alopecia. In general, the skillful evaluation of alopecia usually requires evaluation by a dermatopathologist rather than a general pathologist.
- •
In difficult cases, some dermatologists will perform a trichogram (so-called hair pluck), in which 50 to 100 hairs are pulled and examined to determine the ratio of anagen, catagen, and telogen hairs. This test is painful and requires expertise for interpretation. It is not recommended in the urgent care setting.
Treatment
- •
For men, finasteride (1 mg PO qd) produces improved hair counts of about 9% at 1 year and 15% at 2 years. It is most successful in early-onset androgenic alopecia. It is not nearly as efficacious in older women and should never be used in any woman who can become pregnant.
- •
Topical minoxidil solution (to the scalp, bid) is efficacious. Topical 5% minoxidil has been found to be statistically superior to topical 2% minoxidil in men and women.
- •
Cyproterone acetate is an antiandrogenic agent used in women with androgenic alopecia due hyperandrogenic states.
- •
There is weak evidence that concomitant seborrheic dermatitis may worsen androgenic alopecia, and treatment with 1% pyrithione zinc shampoo or a ketoconazole-based shampoo may decrease hair loss.
- •
Spironolactone (100–200 mg po qd) competitively inhibits androgen receptor binding. The drug does not reverse hair loss but may slow progression. Because of its side effect profile, it can only be used in women and cannot be used by women who may become pregnant because it may feminize a male fetus.
- •
As a last resort, hair transplantation is an option for some patients. However, a hair transplant is a time-consuming, painful, and expensive procedure, with the results being dependent on the skill of the surgeon.
Telogen Effluvium
ICD10 code L65.0
INTERNAL DISORDER
Pathogenesis
Telogen effluvium results from abnormal synchronization of a normal random hair growth cycle. In normal persons, 90% to 95% of the scalp hairs are in anagen (the growth phase), 1% are in catagen (a regressive phase), and 5% to 10% are in telogen phase (a rest phase). In telogen effluvium, a major physical stressor, such as childbirth, marked weight loss, sustained high fever, or a similar event, induces a large number of hairs to transition from anagen to catagen and telogen simultaneously. Hence, there is marked hair loss 2 to 4 months after the physical insult because many hairs enter telogen at the same time.
- •
Childbirth
- •
Endocrinologic changes
- •
High fever
- •
Idiopathic (no cause found in one-third of cases)
- •
Malabsorption syndromes
- •
Medication changes
- •
Surgery (usually major surgery)
- •
Trauma (car wreck with injury)
- •
Weight loss (typically crash diet)
Clinical Features
- •
Telogen effluvium causes an abrupt diffuse hair loss ( Fig. 24.5 ). Patients have described hair as “falling out by its roots.”

Fig. 24.5
Telogen effluvium daily hair counts demonstrating loss of more than 200 hairs/day.
(From the Fitzsimons Army Medical Center Collection, Aurora, CO.)
- •
The hair loss usually occurs 2 to 4 months after a precipitating event ( Figs. 24.6–24.8 ).
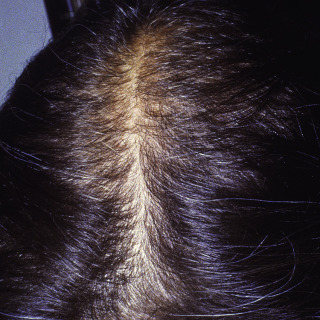
Fig. 24.6
Moderate telogen effluvium demonstrating accentuation of the part.
(From the Fitzsimons Army Medical Center Collection, Aurora, CO.)

Fig. 24.7
Woman with severe telogen effluvium.
(From the Fitzsimons Army Medical Center Collection, Aurora, CO.)

Fig. 24.8
Severe telogen effluvium due to hypothyroidism.
- •
Typically, less than one-third of all hairs are lost.
- •
The scalp appears normal, without erythema or scale, unless a second skin disorder is also present (e.g., seborrheic dermatitis).
- •
Examination of the nails may demonstrate horizontal lines (Beau lines) from the same stressful event that has interrupted nail growth.
Diagnosis
- •
The history of a precipitating cause is important to the diagnosis, but, in some cases, the patient may not report an identifiable event.
- •
If no precipitating event is identified, the patient’s medications should be reviewed. Drugs usually implicated in inducing telogen effluvium include hormone and thyroid replacement drugs, nonsteroidal antiinflammatory drugs (NSAIDs), anticoagulants, beta blockers, systemic retinoids, and some antihyperlipidemia agents.
- •
In cases without a readily identifiable cause, a complete blood count (CBC), serum ferritin level (to rule out iron deficiency), and thyroid function studies should be ordered.
- •
Hair loss should be diffuse, with less than one-third of the hair lost and with a normal scalp.
- •
The presence of Beau lines of the nails is strongly supportive of a diagnosis of telogen effluvium.
- •
A biopsy (4-mm punch biopsy to fat) may suggest the diagnosis, but the result is usually nondiagnostic. A biopsy is useful in excluding other diseases, including scarring alopecia.
Treatment
- •
No treatment other than reassurance is reasonable because most cases are self-limited. Over time, the hair will return to a random growth pattern, and the condition will resolve.
- •
Patients with telogen effluvium due to various systemic perturbations, such as thyroid disease, malnutrition, or anemia, may demonstrate persistent alopecia unless those conditions are rectified.
- •
Rare patients, especially middle-aged women, may develop a chronic telogen effluvium that continues for years. There are few data on the treatment of this rare and persistent variant, but topical minoxidil is the most reasonable treatment approach because it promotes and prolongs the anagen phase.
Trichotillomania
ICD10 code F63.3
PSYCHIATRIC DISORDER
Pathogenesis
Trichotillomania is a neuropsychiatric condition characterized by a compulsion to pull out one’s hair. The compulsion may range from a mild, stress-relieving habit, similar to thumb sucking, to a near maniac and psychotic compulsion that is comorbid with other psychiatric issues. The incidence of trichotillomania is unknown, but the condition is more common in young children and adolescents and in females more than males. Two patterns are recognized— automatic, where hair is pulled nearly inadvertently while the person is engaged in another activity (e.g., watching television, studying), and focused, where hair pulling is the only activity at the time. About 50% of patients play with or chew their hair after pulling it. Some patients swallow the hair, leading to a gastric trichobezoar.
Clinical Features
- •
Irregular patches of nonscarring alopecia may occur anywhere but are most common on the vertex scalp. Some patients may demonstrate scarring from repetitive pulling or from additional psychotic behavior, such as attempting to dig out the hairs.
- •
An important clinical clue is hairs of different lengths in a single area of perceived loss. This results from patients pulling hairs individually, over time, with partial regrowth ( Figs. 24.9 and 24.10 ).










