CHAPTER 36 Alloplastic chin augmentation
Physical evaluation
Lower lip analysis
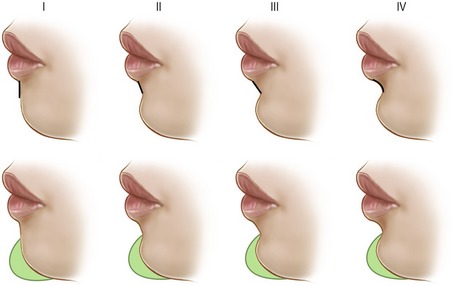
The inclination of the lower lip white roll to labiomental fold affects perception of chin size after augmentation or reduction (Fig. 36.1). If the inclination of the lower lip is vertical and the demarcation between the lip and chin is poor, the patient will appear to have an excessively large chin after augmentation. This is particularly true if a full height implant is incorrectly used. The lower lip analysis is intermingled with the labiomental fold analysis because the lip inclination helps define the labiomental fold. If a patient has a deep overbite and the lip is everted, then the lower lip will have an oblique inclination. The obliquity of the lower lip will contribute to a deeper labiomental fold with a more acute angle. The surgeon should note this because an alloplastic implant that is too tall will deepen the fold and make the labiomental fold angle even more acute. If it is helpful, the lower lip inclination can be classified as follows: Type I is nearly vertical, type II is slightly posterior, type III is significantly posterior, and type IV is most oblique.
Labiomental fold analysis
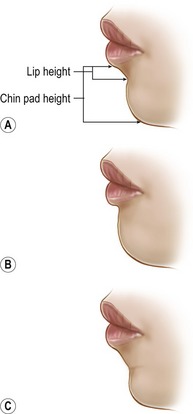
If two chins project exactly the same amount, the chin with the higher and/or shallower labiomental fold will always appear larger from the front (Fig. 36.2). Since the chin is primarily seen as the pad, the labiomental fold defines the apparent vertical height of the chin. Thus, augmenting a patient with a high, shallow labiomental fold tends to increase the appearance of the vertical height of the chin as well as its overall size. To overcome this problem, the surgeon should reduce the vertical height of the implant (see below) to limit augmentation to the lower pogonion. If the chin is long with a high fold, the patient may need both a vertical chin reduction and a sagittal augmentation. In contrast, a patient with a low, distinct labiomental fold will tolerate chin augmentation much better because the implant accentuates only the chin pad.
Static and dynamic chin pad analysis
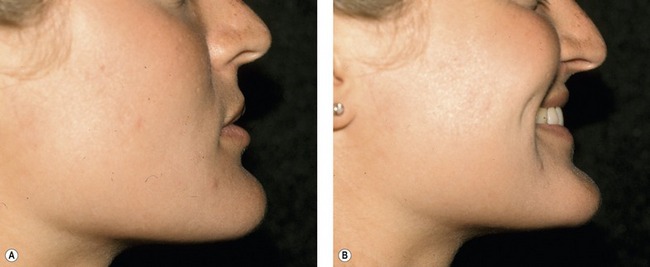
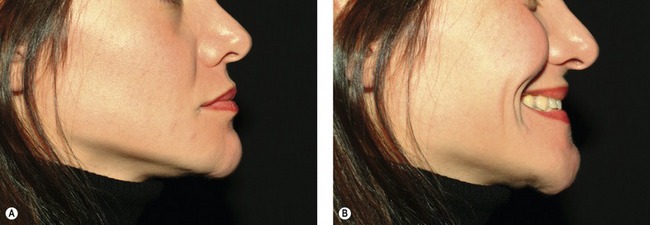
The observer will note that when a chin pad is thick, a smile usually improves the patient’s appearance because the thick pad becomes effaced (Fig. 36.3). In contrast, as a thin chin pad is effaced upon smiling, the chin appears even more prominent (Fig. 36.4). During a normal smile, elevation of the corners of the mouth brings the chin pad superiorly. Some patients have a horizontal non-lifting smile such that the lower lip depressors are unopposed. Unopposed activation of the lower lip depressors produces dynamic chin pad ptosis with smiling as the chin pad drops (Fig. 36.5).
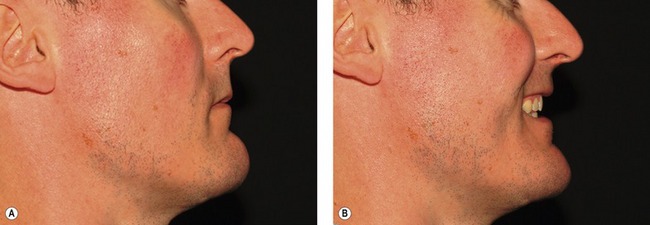
Fig. 36.3 Effect of smiling on a thick chin pad. A, Lateral photograph of patient in repose. B, During a smile, the thick chin pad becomes effaced, usually improving the appearance of the chin.
Submental analysis
During the physical evaluation, the surgeon must keep in mind that chin augmentation in women should be conservative. Female patients are more apt to complain that a chin implant is too large and request removal. It is important to note, that removing an excessively large implant is no simple matter. Removing an implant can result in surface irregularities and fasciculations or the redundant tissue can cause static chin pad ptosis (Fig. 36.6). When evaluating a patient with an excessively large implant, rather than simply removing the implant, we recommend that the existing implant be exchanged with a smaller implant (see below) or an osseous genioplasty should be performed. The new implant or osseous advancement will support the chin pad soft tissues and reduce fasciculations and/or ptosis.

Anatomy
On the labial surface of the mandible in the midline is the symphyseal spine which is also referred to as the surgical spine. The symphyseal spine divides to enclose a triangular eminence called the mental protuberance. The center of the mental protuberance is depressed, but its raised lateral borders form the mental tubercles. On either side of the upper symphysis, just below the mandibular incisors are the incisive fossae. The incisive fossae are the origins of the mentalis muscle. The mentalis muscles coalesce to form the bulk of the chin pad and they insert into the chin pad dermis to maintain lip position in repose and elevate and protrude the lower lip in animation. The mentalis muscles have horizontal and oblique components (Fig. 36.7






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


