Fig. 3.1
The diagram of skin vascular system
- 1.
The direct cutaneous artery originates from the inner arterial trunk, passes out from the deep fascia through the intermuscular space or intermuscular septum, goes along the direction parallel to the skin surface in the subcutaneous tissue in the shallow surface of the muscle, and gives off branches along the way to feed the subcutaneous fat and skin (Figs. 3.2 and 3.3). The blood vessels taking the direct cutaneous artery as the axis can be formed into axial pattern skin flap, such as the circumflex scapular artery, superficial epigastric artery, dorsal pedal artery, and radial artery [7, 8].
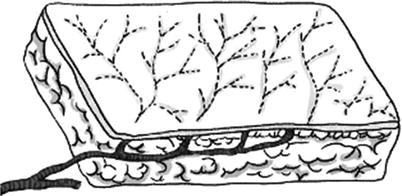
Fig. 3.2
The diagram of skin flap with direct cutaneous artery
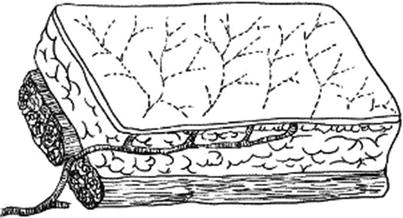
Fig. 3.3
The diagram of skin flap with the cutaneous artery from the intermuscular space
- 2.
Myocutaneous artery: The myocutaneous artery originates from the artery feeding the muscles, which gives off the myocutaneous branch to vertically pass out the deep fascia from the muscle and enter into the above skin tissue to turn into the myocutaneous artery to feed the subcutaneous tissue and skin. The vast majority of human skins cover the muscles, and every muscle has blood vessels; therefore, the myocutaneous arteries are the feeding arteries of the vast majority of human skins. The random pattern skin flaps can be formed through taking the myocutaneous arteries as blood vessels. If the arteries entering into the muscle are taken as the feeding blood vessels, the muscle and the above skin tissue can be harvested concurrently to form the myocutaneous flap (Fig. 3.4).
Fig. 3.4
The diagram of skin flap with the intramuscular blood vessels
- 3.
Deep fascial vascular plexus: The obvious deep fascial vascular plexus exists in the deep fascia and the loose connective tissues above and under the deep fascia. The deep fascial vascular plexuses are more obvious in the limbs, including three layers such as subfascial layer, fascial layer, and epifascial layer, and the epifascial vascular plexus is mostly abundant. The blood supply sources of these vascular plexuses include direct cutaneous arteries, myocutaneous arteries, and the recurrent branches of subcutaneous vascular plexus. When a skin flap is formed in the clinic, if the deep fascia is included, the skin flap becomes a fasciocutaneous flap; its blood supply is more abundant than that of the usual skin flap, and its survival length increases by 15–20%.
- 4.
Subcutaneous vascular plexus: It is located in the superficial fascia; thus, it is also called superficial fascial vascular plexus. The superficial fascia divides the subcutaneous fats into two layers such as superficial layer and deep layer. The superficial layer is denser, and the deep layer is looser. Within this superficial fascia, there exists the vascular plexus going in horizontal direction, and its degree of development varies in different parts of the body, which is more abundant in the body trunk than that in the lower limbs. The superficial fascial vascular plexus has richer anastomoses with the down deep fascia vascular plexus and the above skin vascular plexus, whose blood supply comes from the branches of two kinds of cutaneous arteries. The presence of this vascular plexus is the anatomical basis of the formation of subcutaneous fat flap (Fig. 3.5).
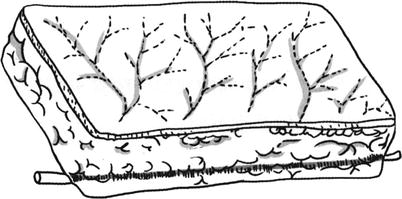
Fig. 3.5
The diagram of skin flap with the main blood vessel plus small branch blood vessels
- 5.
Subdermal vascular plexus: It is located at the junction of the dermis and subcutaneous fat. The vascular plexus is broad and abundant and is the main blood supply system of the skin; many final branches of the two kinds of cutaneous arteries end up in this layer. This vascular plexus gives off many small arteries, the walls of which have continuous smooth muscles, and its main function is to distribute the blood. Some small arteries run obliquely or vertically upward into the reticular dermis or join into the human dermal vascular plexus or continue to run upward and are connected to each other to form into the arch anastomosis; other small arteries run downward to feed the subcutaneous fat and various glands. The subdermal vascular plexus is important for maintaining the blood supply of the skip flap, and it should be protected when the skin flap is formed; otherwise, it is very difficult for the skin flap to survive.
- 6.
Dermal and subepidermal vascular plexuses: The dermal vascular plexus is located in the reticular dermis, while the subepidermal vascular plexus is located between the lower bound of the dermal papilla ridge and the dermal-epidermal line, and the two layers of vascular plexuses provide real blood circulation to the skin. The small artery walls of the dermal vascular plexus have discontinuous smooth muscle components, which mainly have a thermal regulation effect. The subepidermal vascular plexus belongs to the capillaries, whose walls have no smooth muscle, and it mainly has nutritional functions.
1.3 Classification of the Skin Flaps
1.3.1 The Skin Flaps Are Classified According to the Distance Between the Donor Site and the Receptor Site and the Transfer Modes
- 1.
Local skin flap: The local skin flap is the skin flap formed in the adjacent area of the receptor site, which can be further divided into two types such as advancement skin flap and pivot skin flap according to the transfer modes. The advancement skin flap can be pushed forward directly into the receptor site and does not need any rotating or lateral movement. It includes single-pedicle advancement skin flap and double-pedicle advancement skin flap. V-Y skin flap (Fig. 3.6) and Y-V skin flap (Fig. 3.7) also belong to the advancement skin flaps. The pivot skin flap refers to the skin flap which rotates around the pivot point in the skin flap base, and its rotating arc radius is the line of maximum tension of the skin flap. All the rotation skin flap (Figs. 3.8 and 3.9), translocation skin flap, and insertion skin flap belong to the pivot skin flaps. The standard rotation skin flap is generally semicircular. The translocation skin flap is generally rectangular, and the rhomboid skin flap, bilobed skin flap, and the skip flap formed after Z-plasty also belong to the translocation skin flaps. The rotation skin flap is not as closely proximate to the defect area as the translocation skin flap and the insertion skin flap. There are normal tissues between the rotation skin flap and the defect area, and the rotation skin flap must cross over the top of the adjacent tissue or pass through underneath the adjacent tissue to reach into the defect area during the transfer.

Fig. 3.6
The use of V-Y skin flap to correct the slight ectropion of lower eyelid

Fig. 3.7
The use of V-Y skin flap to correct the slight ectropion of lower eyelid
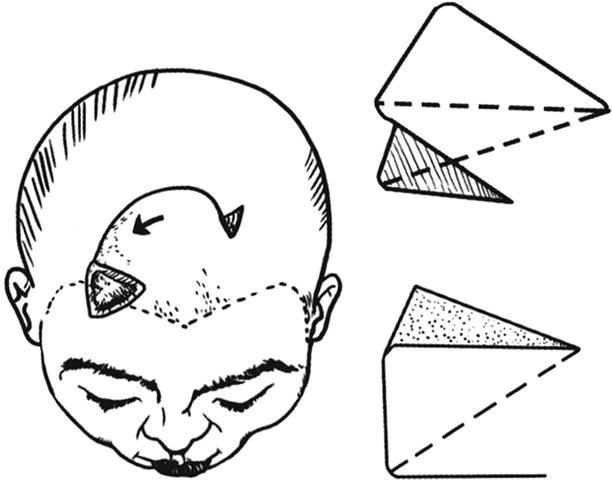
Fig. 3.8
The design of the rotation skin flap (1)
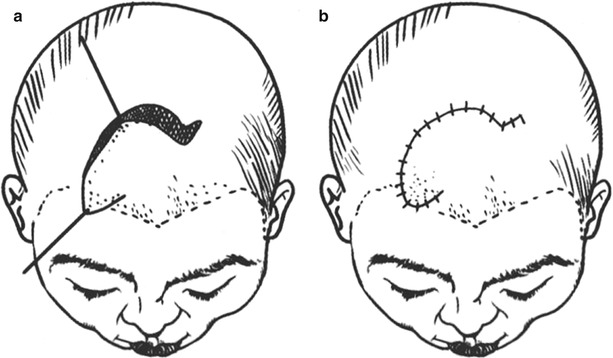
Fig. 3.9
The design of the rotation skin flap (2)
- 2.
Distal skin flap: The skin flap formed in the distant site away from the receptor site is called the distal skin flap. Such skin flaps can be transferred into the receptor sites using direct and indirect methods or with vascular anastomosis. The skin flap which is directly transferred is called the direct distal skin flap, such as the cross-leg skin flap and the abdominal pedicled skin flap which is transplanted to the back of the hand; the skin flap which is indirectly transferred is called the indirect distal skin flap, such as abdominal pedicled tubular skin flap which is transferred into the face and neck wounds using the wrist carrying method; the skin flap which is transferred by means of vascular anastomosis is called the free skin flap, such as the dorsalis pedis skin flap which is transplanted to the back of the hand; in addition to that, the distal skin flap is transferred by means of vascular anastomosis; in general, it is needed to carry out operations for more than two times to complete the entire transplantation process of the distal skin flap.
1.3.2 The Skin Flaps Are Classified According to the Blood Supply Types
The skin flaps can be divided into two types such as the skin flaps supplied with blood by the myocutaneous artery and the skin flaps supplied with blood by the direct cutaneous artery according to the blood supply types. The skin flaps with the myocutaneous artery can be further divided into two types such as random skin pattern flap and myocutaneous flap; the skin flaps with the direct cutaneous artery refer primarily to the axial pattern skin flap. The myocutaneous flaps and the axial pattern skin flaps can only be formed in some specific areas.
1.3.3 The Skin Flaps Are Classified According to the Composition
The skin flaps can be divided into simple skip flap and compound skin flap according to the composition. The compound skin flap includes fasciocutaneous flap, myocutaneous flap, osteocutaneous flap, and neurosensory skin flap. The simple skip flap only contains skin and subcutaneous tissue, and it will be called the fasciocutaneous flap if the deep fascia is also included. The myocutaneous flap is the skin flap including muscles; if the skip flap contains bone tissues, it will be called the osteocutaneous flap. The neurosensory skin flap refers to the skin flap including cutaneous sensory nerves.
1.3.4 The Skin Flaps Are Classified According to the Anatomical Features and Clinical Application Methods of the Blood Supply of the Skin Flap
- 1.
Axial pattern skin flap: It has been described in detail in Sect. 3.4 of this chapter, and thus it will not be repeatedly described here.
- 2.
Prefabricated axial pattern skin flap: The donor sites of the human axial pattern skin flaps are limited after all. The skins in some areas have good textures and hidden locations, but don’t have an ideal axial blood vessel. The prefabricated skin flap refers to that an axial blood vessel is artificially implanted into the area under a non-axial pattern skin flap, and then after a period of time, when the implanted axial blood vessel is linked up with the skin blood supply, it can be used as axial pattern skin flap. Shen Zuyao et al. transplanted the greater omentum into an area under the abdominal skin and used the right gastroepiploic blood vessel as the pedicle to make the omental axial pattern skin flap. The temporal vascularized skin flap designed by Chen Baoju et al. is that at the superficial surface of the superficial temporal blood vessels, the scalp is cut open and lifted up, and then it is folded and sutured, and the skin transplantation is performed within the distribution area of the superficial temporal blood vessels; after the transplanted skin graft survives, it will be harvested together with the superficial temporal blood vessels for free transplantation, and the folded scalp will be separated again and sutured back into the previous place The research and application of such prefabricated axial pattern skin flap open up a new source for free skin flap transplantation.
- 3.
Combined skin flap: When it is required to repair some soft tissue defects in an extra-large range or repair two skin flaps with different functions (or other tissue flaps) in the defect area at the same time, this is not a problem which can be solved only by a single skin flap or myocutaneous flap. The combined skin flap is that two free skin flaps with independent vascular pedicles are connected to form an assembly with a common vascular pedicle using the method of vascular anastomosis method, in order to repair some extensive and complex wounds. For example, the latissimus dorsi myocutaneous flap is connected with a finger (toe) nail skin flap to repair the large-area skin defect in the thumb, palm, and volar forearm; or the latissimus dorsi myocutaneous flap is connected with the fibula to repair the calf skin defect combined with a large tibial defect. If the latissimus dorsi myocutaneous flap is used to be connected with other skin flaps, the vascular pedicle of the latissimus dorsi myocutaneous flap can be separated from the thoracic dorsal blood vessel to the subscapular blood vessel, whose branch circumflex scapular blood vessel is anatomized with the vascular pedicles of other skin flap. If the forearm skin flap is used to be connected with other skin flaps, the distal end of the main blood vessel is anastomosed with the vascular pedicle of another skin flap using the characteristics of the radial blood vessels running through the entire length of the skin flap. The former is called the bridge flap, while the latter is called the terminal flap, and this combination is also known as the two tandem skin flaps. Due to the composite application of the skin flap and myocutaneous flap, the repair of severe trauma has reached a new technological level [9–11].
- 4.
Venous skin flap: The venous skin flap is a new type of skin flap with nonphysiological blood circulation. In recent years, the scholars at home and abroad consider that the blood flow can also make the skin flap survive only through the venous approach after conducting the experimental studies and clinical applications of venous skin flaps, of which, there are venous skin flaps nourished by the venous blood, and there are also venous skin flaps nourished by arterial blood. The emergence of the venous skin flaps has changed the traditional concept that the conventional free skin flap must have a complete set of arterial and venous systems. The advantages of the venous skin flaps include (1) which can avoid sacrifice of an artery in donor site and receptor site; (2) the subcutaneous superficial vein has a thick diameter and a constant location, which is visible to the naked eye and is easy to dissect and anastomose; and (3) many subcutaneous vein networks make the donor sites of the skin flaps more extensive. Although the venous skin flaps have the above advantages, the hemodynamic change and survival mechanism of the skin flap are not yet very clear, and there is also no lack of failure examples in various reports. Therefore, the venous skin flaps are still in the stages of experimental studies and clinical trials, and many problems remain to be further explored.
1.4 The Selection of the Skin Flaps
The skin flaps are available in each part of the body. A defect site can be repaired selectively using a variety of skin flaps. Whether the selection of the skin flap is correct determines the success of the surgical repair; therefore, it should be considered based on the situations in donor site and receptor site, the degree of operation difficulty, the patient’s tolerance, and the surgeon’s familiarity degree for skin flap harvesting. The selection of the skin flaps and the surgical design should follow the principles from simple to complex, safe, reliable, and effective.
1.4.1 The Ortho-position Skin Flap Is Preferably Selected to Repair the Receptor Site
Since the color, texture, and thickness of the adjacent skin are close to those of the receptor site, and the transfer is convenient, the ortho-position skin flap should be preferred firstly. For example, the scapular skin flap and lateral thoracic skin flap are selected for repair of axillary skin tissue defects, and the neck platys myocutaneous flap is selected for repair of defects in maxillo-cervical area.
1.4.2 The Myocutaneous Flap Is Selected to Repair the Receptor Site with Deeper Tissue Defects or Severe Infection
The myocutaneous flap has a large volume of tissue and a rich blood supply, and it can fill the defects and has strong resistance to infection. For example, the latissimus dorsi myocutaneous flaps are selected for repairs of the wounds of serious electrical burns or chronic ulcers.
1.4.3 The Skin Flap Is Selected According to Functional Needs of the Receptor Sites
- 1.
The medial plantar island skin flap is preferred for repair of heel defects, and the heel will have both feeling and rub resistance after the repair.
- 2.
The burn injury in the upper arm can cause biceps or triceps necrosis. It is not only needed to repair the skin defects, but also is needed to reconstruct the functions of elbow flexion and extension of the biceps or triceps. The latissimus dorsi myocutaneous flap with nerves is used, and the latissimus dorsi muscle is used to replace the biceps or triceps to restore the functions of elbow flexion and extension.
- 3.
When the Achilles tendon is burnt and necrotized, it will be repaired by free transplantation of the tensor fasciae latae myocutaneous flap, and part of the fascia lata femori is formed into a roll to reconstruct the Achilles tendon, which can achieve a good effect.
- 4.
When there is a concurrent bone defect and malformation, the osteocutaneous flap is used to reconstruct the bone defects.
- 5.
The dorsalis pedis skin flap with extensor digitorum longus is used to repair the tendon defects in the wrist area.
1.4.4 The Skin Flap Is Selected According to Blood Supply Sources
The skin flaps supplied with blood mainly by a branch artery are selected. It is avoided as far as possible to sacrifice the main blood vessels of the limbs.
1.5 Transplantation Methods of Skin Flaps
The harvesting of axial pattern skin flap is not restricted by the length-to-width ratio; as long as it is designed within the supply scope of the axial pattern blood vessel, the skin flap will not be necrotized. Its clinical use is more flexible than that of the random pattern skin flap, and two methods such as local transfer and free transplantation can be formed. During the local transfer, the pedicle can carry some skins (peninsula shaped); the blood vessel can also be completely dissociated, and an island-shaped skin flap is formed, the rotating radian is big, and it is easy to be transferred; the free transplantation requires vascular anastomosis; thus, the operation is slightly complicated.
1.5.1 Pedicled Transfer
The pedicled transfer is divided into two modes such as adjacent transfer and distal transfer according to the defect sites. For example, the defects in the wrist area are often repaired with the distal iliolumbar skin flap with pedicled superficial iliac circumflex blood vessel; the iliolumbar skin flap can be formed into various shapes according to the need of hand defects, and the operation method is simple, which is convenient to be used in the grassroots units. The disadvantage is that it requires reoperation at 3 weeks after operation to cut off the pedicle. The adjacent transfer of the island-shaped skin flap is more flexible, for example, the island-shaped latissimus dorsi myocutaneous flaps with pedicled thoracic dorsal arteriovenous vessels can repair the defects in occipitalia, the top of the head, face, neck, chest, and upper limbs to the wrist area. In order to increase the length of the trip of the skin flap, when the defects in the head and neck are repaired, the skin flap penetrates out from underneath the pectoralis major muscle, which can increase the length of 5–6 cm.
There are more than 70 skin flaps and myocutaneous flaps in various parts of the body; in general, the skip flap is harvested at the nearest site, which is simple and operable. In terms of repair and reconstruction, as long as the surgeons are familiar with the commonly used skin flaps (Table 3.1) and can flexibly use them, the needs can be basically met. For multiple regional injuries in upper limb, when it is difficulty to repair them with a skin flap, the multiple skin flaps and combined skin flap can be used to repair them, for example, the latissimus dorsi myocutaneous flap combined with the lateral thoracic skin flap is used to repair the defects in wrist and palm of the forearm, and the latissimus dorsi myocutaneous flap combined with the iliolumbar skin flap is used to repair the circumferential soft tissue defects in elbows and forearms. The extensive and circular wound from elbow to wrist can be repaired with the huge thoracoabdominal skin flaps. The paraumbilical blood vessels and the lateral cutaneous branches of intercostal blood vessels are taken as the axes; when the thoracoabdominal skin flap is harvested, the lower boundary of the skin flap is located underneath the iliac crest in the groin to the lateral border of sacral rectus in the waist and along the axillary line to the tenth intercostal space; the medial side of the skin is located at the midline of the rectus abdominis muscle up to the umbilical region. Attention is paid to protect the cutaneous branch of the paraumbilical blood vessel, the skin flap is separated and lifted, the forearm is placed at the thoracoabdominal area, and then the wounds in the forearm and wrist are wrapped with the skin flap. A part of the wound in the inner side of the forearm is not wrapped with the skin flap, which clings to the surface of muscle membrane of the obliquus externus abdominis muscle, and it will be covered with an appropriate length of skin which is harvested at the pedicle site when the pedicle is cut off.
Table 3.1
Pedicled transfer and repair of commonly used skin flaps and myocutaneous flaps
Names of skin flaps | Main axial pattern blood vessels | Repair sites |
|---|---|---|
Forehead skin flap | Superficial temporal artery | Face, cheekbone, mouth floor |
Head skin flap | The parietal branch of the superficial temporal artery or the occipital artery | The top of the head |
Neck platysma myocutaneous flap | Facial artery, superior thyroid artery, transverse cervical artery | Jaw, neck, chin |
Trapezius myocutaneous flap | Transverse cervical artery | Neck, jaw |
Deltopectoral skin flap | The perforating branch of internal thoracic artery | Face, jaw, neck |
Pectoralis major myocutaneous flap | Thoracoacromial artery | Neck, jaw |
Latissimus dorsi myocutaneous flap | Thoracodorsal artery | Occipitalia, the top of the head, face, neck, shoulder, prethoracic area, upper arm, forearm |
Scapular flap | Circumflex scapular artery | Shoulder, armpit, upper arm |
Lateral thoracic skin flap | Lateral thoracic artery | Armpit, chest wall |
The iliolumbar skin flap | Superficial epigastric artery, superficial iliac circumflex artery | Perineum, penile reconstruction, hand (pedicled transfer) |
Forearm skin flap | Radial artery | Hand (retrograde transfer) |
The dorsal skin flap of index finger | The first dorsal metacarpal artery | Thumb, thumb web |
The tensor fasciae latae myocutaneous flap | Lateral femoral circumflex artery | Lower abdominal wall, groin |
Transverse rectus abdominis myocutaneous | Superior epigastric artery, inferior epigastric artery | Chest wall, groin, inner thigh |
The medial crural skin flap | Posterior tibial artery | Knee, upper calves |
Gastrocnemius myocutaneous flap | Sural artery | Knee, pretibial area |
Dorsalis pedis skin flap | Dorsal pedal artery | Ankle area, heel, pretibial area |
Medial plantar skin flap | The medial plantar artery | Heel, ankle area |
Anterolateral femoral skin flap | Femoral anterolateral artery | Groin, perineum, knee (retrograde transfer), upper pretibial area |
Saphenous artery flap | Saphenous artery | Groin, perineum, oberschenkel, pretibial area, knee |
It is supposed to keep limb length to the greatest extent for the patients with amputation, and the defect wound in the stump should be covered with the skip flap. Especially for the upper limbs, retaining the elbow joint, shoulder joint, and a certain length of the radius, ulna, and humerus has an important significance for retaining the limb function and assembling the prosthesis. For the limb necrosis with deep burn wound in the armpit, sometimes it is necessary to perform the shoulder joint disarticulation to repair the defect wound in the stump. In order to preserve shoulder joint and the length of the part of the humerus, the stump of the humerus is implanted subcutaneously in the lateral chest, and the axillary wound is directly sutured and closed after adduction of the shoulder joint. A month later, the lateral thoracic skin flap is separated and lifted to partially repair the stump, and the axillary scar release is carried to produce shoulder abduction, and the skin graft transplantation is performed for the wound fault.
1.5.2 Free Skin Flap Transplantation with Vascular Anastomosis
Some wounds which cannot be repaired with pedicled skin flap transfer can only be repaired with free skin flap. Since the free skin flap needs vascular anastomosis, the surgeons are required to have a certain operation techniques under microscope. The key to success is the quality of vascular anastomosis surgery and performing vascular anastomosis at the site of the originally damaged blood vessels. The high-voltage electrical burns are often accompanied by varying degrees of vascular injuries, and the location of the vascular anastomosis should be 3–5 cm away from the damaged site. The surgical microscope observation shows that the blood vessel endangium is smooth and slippery without exfoliation and obvious edema, and thus it is more reliable to perform vascular anastomosis here. For larger wounds or the receptor sites without blood vessels available for anastomosis, the following methods may be taken:
- 1.
Tandem skin flap: The tandem skin flaps can only include the vascular network skin flaps with blood vessel branches of the arterial stems, such as the radial artery forearm skin flap, dorsalis pedis skin flap, and medial crural skin flap. The distal blood vessels are anastomosed with the blood vessels in another piece of skin flap, and two skin flaps are connected together to repair a larger wound.
- 2.
Combined skin flap: The combined skin flaps have the same vascular pedicle, for example, the latissimus dorsi myocutaneous flap is combined with the scapular skin flap; thus, the dissection is performed from the subscapularis artery. Because the subscapularis artery from the axillary artery is divided into the circumflex scapular artery and the thoracodorsal artery to feed the scapular skin and the latissimus dorsi muscle, respectively, the skin in the entire shoulder and back area and the latissimus dorsi muscle can be resected.
- 3.
The bridge-like cross-skin flap with vascular anastomosis: For transplantation of the bridge-like cross-skin flap with vascular anastomosis, if there are no blood vessels in the receptor site available for anastomosis, the blood vessels in the contralateral normal limb can be used for anastomosis. If there is a large soft tissue defect in the lower leg of one side, the axial pattern blood vessel of the skin flap can be anastomosed with the posterior tibial vessel or the pretibial blood vessel in the lower leg of the other side to form a bridge-like repair of contralateral limb defect.
- 4.
Transplantation of carried free skin flap: In the past, the wrist-carried skin tube is often used to repair the distal wound, since the formation time of the tubular skin flap is longer. It is not suitable for immediate repair of the wound defect. Now it has been rarely used. However, in some special patient cases, if the local damage is more severe, which cannot be repaired by other methods, the wrist radial artery and cephalic vein can also be taken as the blood vessel for anastomosis in receptor site to carry free skin flap or myocutaneous flap to repair the wound defect in sites such as the groin, abdominal wall, or contralateral upper limbs.
After transplantation of the bridge-like cross-free skin flap and the wrist-carried tubular skin flap, it is needed to fix the limb for 3–4 weeks and then cut off the pedicle; meanwhile, the original blood vessels (posterior tibial artery and radial artery) are anastomosed again to ensure an adequate blood supply to the limb.
1.5.3 Transplantation of Superthin Skin Flap
The superthin skin flap is the subdermal vascular network skin flap. The excessive subcutaneous adipose tissue in the skip flap after dissociation is cut off; while the subdermal vascular network and the fat with the thickness of 2–3 mm are retained, and the pedicle area is lightly thicker, then the skip flap is extended and the subdermal vascular network can be observed. The advantages of this skin flap are that the appearance is not significantly bloated; the time for cutting off the pedicle can be advanced, as early as 10 days or so; and the pedicle can be cut off. But for the tendon-exposed wound with aponeurosis damage, after the transplantation of the superthin skin flap, the muscle tendon is adapted to be adhered to the subcutaneous tissue and, thus, affecting the functional activity; therefore, it is best to cover a layer of deep fascia on the muscle tendon without aponeurosis; thus, the muscle tendon has a certain sliding function in the movement. Only the skin flap with the deep fascia flap can achieve these results.
1.6 Monitor of Blood Circulation After Skin Flap
Good blood circulation is a basic condition for skin flap survival; therefore, monitoring the status of blood circulation flap will be of great importance in determining the time of cutting off the pedicle for the pedicle skin flap, confirming whether the delayed skin flap is safe, judging the prognosis of skin flap, and early detecting the vascular crisis. There are a variety of testing methods for skin flap blood circulation, and they can be divided into two broad types such as objective and subjective tests.
1.6.1 Subjective Test
- 1.
Color change: Compared with before transplantation, if the skin flap becomes obviously pale, it indicates the insufficient arterial blood supply; if the skin flap becomes purple, it indicates the venous reflux obstacle. Because there is a big difference in skin colors in different parts of the body, it is not very reliable to judge the blood circulation according to the changes in the color of the skin flaps.
- 2.
Capillary refill test: The capillary refill test is one of the microcirculation detection methods commonly used in clinic. Gently press the skip flap with the fingers or the mouth of the test tube, so that the local skip flap is pale; if the blood capillaries are immediately filled after decompression, it indicates good blood circulation; if the blood capillaries are filled slowly, it indicates poor blood circulation. But if the test is applied in the patients with pale skin flap, it is often difficult to judge the situation of the capillary filling. Moreover, even if the skin flap is completely dissociated, sometimes the phenomenon that the skin flap becomes pale after compression and the blood capillaries are filled after decompression can also occur. Therefore, this test has its limitations.
- 3.
Puncture bleeding test: Puncture the skin flap with 18-gauge hypodermic needle or the 11-gauge hypodermic needle to observe the bleeding status; if there is no bleeding, it indicates the poor arterial perfusion; if the bleeding is bright red, but it is more slowly, it indicates that there is some degree of arterial spasm; if the bleeding is active and bright red, it indicates normal arterial perfusion or some degree of congestion; if the bleeding is dark purple, it indicates venous reflux obstacle.
1.6.2 Objective Test
- 1.
Measurement of percutaneous partial pressure of oxygen: The partial pressure value of oxygen in the skin is closely related to its blood supply; if there is a good blood supply, the oxygen partial pressure is high; otherwise the oxygen partial pressure is low. Therefore, the use of transcutaneous partial pressure meter of oxygen to monitor the oxygen partial pressure change in the skin flap is conducive to determining the condition of the blood circulation. The method has the advantages of noninvasiveness and allowing continuous observation, but its application is limited by the high price.
- 2.
Tissue pH measurement: When the tissue hypoxia exists, the anaerobic metabolism is strengthened, and the local lactic acid is accumulated, leading to decreased pH value. Therefore, monitoring the pH changes within the skin flap can judge indirectly its blood supply and prognosis. When the pH within the pedicled skin flap is decreased down to 0.35, the skin flap necrosis will occur.
- 3.
The ultrasound and laser Doppler flowmeter examination: The former can be used to determine the blood flow condition of the axis blood vessel within the axial pattern skin flap, and the latter can be used to detect the microcirculation status of 1 mm3 tissue within the depth of 1.5 mm under the skin surface. Both are noninvasive detection technologies for continuous observation, but the instruments are expensive, and it is required that the examinators have certain experiences.
- 4.
Temperature measurement: At the same external conditions, the temperature of the skin depends primarily on its blood supply; therefore, measuring the temperature of the skin flap can indirectly judge its blood circulation state. The commonly used instruments include infrared temperature instrument and thermocouple thermometer. The temperature measurement types mainly include surface temperature measurement and temperature difference measurement. It is reported that if the surface temperature in the central part of the free skin flap is 3 °C lower than that in the nonsurgical skin, it indicates the formation of the arterial thrombosis; if it is decreased by 1 ~ 2 °C, it indicates the formation of venous thrombosis. It is also reported that if the absolute temperature is below 30 °C after skin flap transplantation, it indicates the occurrence of vascular crisis. Some experimental studies have shown that if the surface temperature of the pig skin flaps is 2.4 °C lower than that of normal skin, it indicates the vein occlusion; if it is decreased by 2.6 °C, it suggests the artery occlusion. The temperature difference measurement is mainly used to determine the patency of anastomosed blood vessels within the transplanted free tissues. The specific detection method is to sew the thermocouple electrodes into both sides of the arterial anastomosis site and record the temperature difference. If the temperature difference is more than 32 °C, it suggests the occurrence of vascular crisis.
- 5.
Other monitoring methods: The optical plethysmograph can be used to measure the tissue blood flow of the skin within the depth of 1–1.5 mm and help determine that the blood supply disorder of the skin flap is arterial disorder or venous disorder. The basic principle of the clearance test is to inject a substance into the skin, and then observe its clearance rates occurring over time, thereby to determine the blood circulation status in the skin flap. There are also methods such as sodium fluorescein staining in vivo, electromagnetic blood flow measurement, microvascular imaging, radioactive microsphere measurement, and in vivo microscopic examination.
2 Random Pattern Skin Flap
2.1 The Blood Supply of the Random Pattern Skin Flap
The arterial blood supplies of the random pattern skin flaps include three sources:
- 1.
Direct cutaneous artery: The artery originates directly from the arterial trunk, passes through intermuscular space and fascia and reaches the subcutaneous adipose layer, and then is incorporated into the subdermal vascular network. This kind of artery only supplies blood to the skin tissue, which is called direct cutaneous artery.
- 2.
Myocutaneous artery: The myocutaneous artery originates from the arterial trunk; enters into the muscle; gives off branches within the muscle, of which, some branches give off branches progressively; passes through the perimysium and enter into the endomysium to form microcirculation; and provides blood supply to muscles. Other branches are the branches of the intramuscular perforator. They go out of the muscles, pass though the deep fascia, and reach to the subcutaneous adipose tissue layer. The calibers of the myocutaneous perforators are relatively small. They repeatedly give off branches in the subcutaneous adipose tissue layers and anastomose with other arterial branches to constitute subdermal vascular network and dermal vascular network.
- 3.
Mixed artery: The mixed artery refers to that after being given off from the deep arterial trunk, the artery is divided into the muscular branch and the cutaneous branch immediately to feed the muscle and skin tissues, respectively, and the two are not interlaced with each other. The skin flap is provided with blood by the pedicle to maintain its metabolism in the transfer process. If its blood supply comes from the direct cutaneous branch or the cutaneous branch of the mixed artery, this kind of skin flap is called axial pattern skin flap. If its blood supply comes from the musculocutaneous perforator of myocutaneous artery, this kind of skin flap is called the random pattern skin flap. Because the caliber of the myocutaneous perforator which feeds the random pattern skin flap is smaller, it cannot be used for bonding anastomosis, and thus the pedicle of the skin flap is required to keep connected with the donor site, so that the blood circulation of the skin flap is uninterruptedly operated. This transfer is called pedicled transplantation, and such skin flap is called the pedicled skin flap.
2.2 The Indications for Random Pattern Skin Flap Transplantation
The random pattern skin flap contains the adipose tissues, and the pedicle supplies blood to the skin flap tissue to maintain its blood circulation and metabolism, and the random pattern skin flap has functions such as repairing the skin tissue defects, resisting the infection, improving the blood supply of the receptor site, and preventing the adhesions and filling sunken defect. After healing, the skin color and texture will not be changed, and no shrinkage will occur at late stage, which is the most widely used means for tissue repair. It is mainly applied to:
- 1.
Repair of perforating defects
- 2.
Organ reconstruction, such as reconstructions of the ear, nose, fingers, and external genitals
- 3.
Repair of deep wounds with exposed important tissues, such as repairs of wounds with exposed bones, joints, cartilages, muscles, and important blood vessels
- 4.
Repair of wound in the place where there exists friction and extrusion, such as repairs of the heel ulcers and bedsores
- 5.
Repairs of wounds with poor blood supply, such as repairs of radiation ulcers and osteomyelitis-induced chronic ulcers
2.3 Classification of Random Pattern Skin Flaps
2.3.1 Classification According to the Sites Where the Skin Flaps Are Formed
The random pattern skin flaps can be divided into head skin flap, skin flap, chest skin flap, back skin flap, abdominal skin flap, upper arm skin flap, and lower limb skin flap according to the sites where the skin flaps are formed.
2.3.2 Classification According to the Relationship Between the Skin Flap Donor Site and Receptor Site
According to the relationship between the donor site and receptor site of the skin flap, the random pattern skin flaps can be divided into:
- 1.
Local skin flap
- (a)
Neighboring skin flap: The donor site is adjacent to the receptor site, but both are separated by normal skin tissue.
- (b)
Ortho-position skin flap: The donor site is connected to the receptor site.
- (a)
- 2.
Distal skin flap
- (a)
Direct skin flap: The donor site and the receptor site are not at the same anatomic site, but the skin flap is transferred directly from the donor site to the receptor site without passing through the intermediate station. For example, the abdominal skin flap is directly transferred to repair the skin tissue defect in the forearm. If one side limb is the donor site, and the skin flap after formation is directly transferred to repair the wound in the other side limb, this kind of skin flap is called cross-skin flap.
- (b)
Indirect skin flap: The skin flap is transferred to the intermediate station; after the blood circulation between the skin flap and the intermediate stations is established, the skin flap carried by the intermediate station is transferred to the receptor site. For example, in order to repair the skin tissue defect in the head with the abdominal skin flap, it is needed to suture one end of the skin flap with the forearm (intermediate station); after the blood supply which is sufficient to feed the skin flap is established, the abdominal skin flap carried by the forearm is transferred to receptor site in the head.
- (a)
2.4 Classification According to the Shape of the Skin Flap
The random pattern skin flaps can be divided into rhomboid skin flap, triangular skin flap, tongue-shaped skin flap, bilobed skin flap, flat skin flap, and tubular skin flap (skin tube) according to their shapes.
2.5 Classification According to the Pedicle Situation
The random pattern skin flaps can be divided into single-pedicle skin flap, double-pedicle skin flap, and subcutaneous pedicle skin flap (the skin tissues around the skin flap are cut open, but the subcutaneous tissues are not exfoliated and are taken as the pedicle of skin flap).
2.6 Classification According to the Subcutaneous Tissue Layers Contained in the Skin Flaps
According to the subcutaneous tissue layers contained in the skin flaps, the random pattern skin flaps can be divided into:
- 1.
Fasciocutaneous flap: The fasciocutaneous flap is the skin flap containing various layers of tissues from the skin to the deep fascia.
- 2.
Subdermal vascular network skin flap (thin skin flap): The subdermal vascular network skin flap only contains the skin and subdermal vascular network, as well as the thin adipose tissue which is reserved for the protection of vascular network.
- 3.
Traditional skin flap: The traditional skin flap refers to the skin flap containing various layers of tissues from the skin to the superficial surface of the deep fascia.
2.7 The Principles for the Design of Random Pattern Skin Flap
The nutritional metabolism of the random pattern skin flap is completed by the blood which passes through the pedicle to enter into the subdermal vascular network and dermal vascular network, and the blood supply of the pedicle comes from the myocutaneous perforator of the myocutaneous artery. These myocutaneous perforators have small calibers, low perfusion pressure, and limited supply scope, in order to ensure that the skin flap has no blood supply disorder in the transfer process and can survive successfully and get good curative effect. When the donor site is being selected and the skin flap is being designed, certain principles should be abided by.
2.7.1 Principles for Selection of Donor Sites
- 1.
The donor site of the skin flap should be selected in the adjacent area of the receptor site. The skin color and texture are similar. The number of operations is less, and the operation is relatively simple.
- 2.
It is not allowed to cause the dysfunctions and morphological abnormalities in the donor sites after harvesting of the skin flap. The functional sites of the joints and the exposed sites are generally not selected as the donor sites.
- 3.
The local skin tissues are normal, and there are no acute and chronic inflammations or other skin lesions.
2.7.2 Principles for Skin Flap Design
- 1.
Appropriate length-to-width ratio: During the transfer, the blood supply maintaining the nutritional metabolism of the random pattern skin flap is completely dependent on the subdermal vascular network from the pedicle, but the scope of perfusion is limited. If the formed skin flap exceeds the scope of perfusion, the skin flap will have ischemic necrosis. According to the clinical practice experience, the ratio of the length of the skin flap to the width of the pedicle should generally not be more than 1.5:1. The length-to-width ratio of the skin flap should better be 1:1 in the sites such as the lower extremities; but the length-to-width ratio of the skin flap can exceed the limit of 1.5:1 in the sites such as head and neck with rich blood supply; sometimes, when the length-to-width ratio of the skin flap is up to 3:1, no blood supply disorder has occurred. If the length-to-width ratio of the designed skin flap exceeds the limit of 1.5:1, it is appropriate to perform skin flap delay at first.
- 2.
Comply with the directions of the blood vessels: The skin flap is designed along with the direction of the blood vessels as much as possible. The pedicle is located in proximal end of the blood vessel. The torso midline is generally located in the blood vessel-lacking area. When designing the skin flap, we should try to avoid exceeding the torso midline.
- 3.
Adopt the reverse design method: A piece of paper is sheared into a figure of the skin flap according to the shape of the tissue defect wound, whose area is slightly larger than the actual defect area. The paper figure of the skin flap is placed in the donor site, and the pedicle of the paper figure of the skin flap is fixed. It is experimented that the skin flap is lifted and transferred to observe whether the pedicle position of the skin flap is appropriate and the direction of the formed skin flap is suitable. In the transfer process, it is required that the skin flap has no tension and the pedicle has no excessive distortion. After the transfer of the skin flap, if the tension is too large and the pedicle is excessively distorted, these are common causes of blood supply disorders occurred after transfer of random pattern skin flap. The adjustment is repeatedly carried out until the satisfaction is achieved, and then the methylrosanilinium chloride is used to mark the location.
There are several things that we should pay attention to:
- (a)
When a local rotation skin flap is designed, particular attention should be paid to that the distance between the rotation pivot point of the skin flap and the farthest point of the skin flap must be greater than or equal to the distance between the rotation pivot point of the skin flap and the farthest point of the defect wound; otherwise, the skin flap will not be able to successfully repair the wound after transfer.
- (b)
When a distal direct skin flap is designed, it is needed to attach the paper figure of skin flap onto the receptor site, and then the receptor site-carried paper figure is matched with the donor site. It is experimentally detected where the best position of the pedicle in the donor site is, so that the skin flap can be transferred to repair the wound most successfully, and the patient will also feel more comfortable. After the pedicle is determined, and then the pedicle of the paper figure of the skin flap is fixed, the paper figure is spread out onto the donor site, and the specific location of the skin flap is marked.
- (c)
When a distal indirect skin is designed, the pedicle of the paper figure of the skin flap should be fixed with intermediate station and is carried to the donor site and the receptor site. The steps for transfer of skin flap are repeatedly rehearsed, and the pedicle position of the skin flap and the direction to form a skin flap are selected.
- (a)
- 4.
The designed skin flap should be greater than the skin flap in the wound; the skin flaps after harvesting usually have a certain degree of contraction; therefore, it is designed that the area of skin flap in the donor site should be greater than the area of the wound in the receptor site by 10–15%, in order to prevent occurrence of the tension after transfer and suture which will affect the blood supply.
2.8 Local Skin Flap Transplantation
The skin flap formed by the skin tissue around the receptor site is called the local skin flap, which has advantages that the skin color and texture are in consistency with those of the receptor site; the transfer operation of the skin flap is simple and convenient, and the transfer and repair can be completed in one operation, and it is the most commonly used skin flap transplantation.
2.8.1 Advancement Skin Flap
The advancement skin flap is the skin flap formed in the adjacent site of the defect wound; after the skin flap is stripped off, it is advanced into the defect area through sliding to repair the wound, and it is also known as the sliding skin flap (Figs. 3.10 and 3.11).
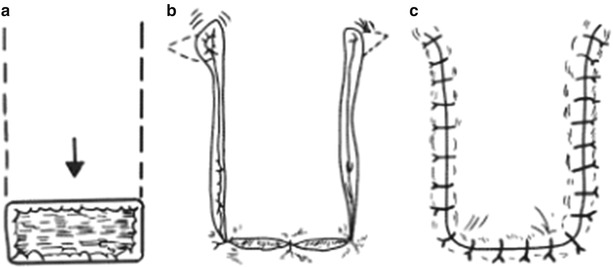
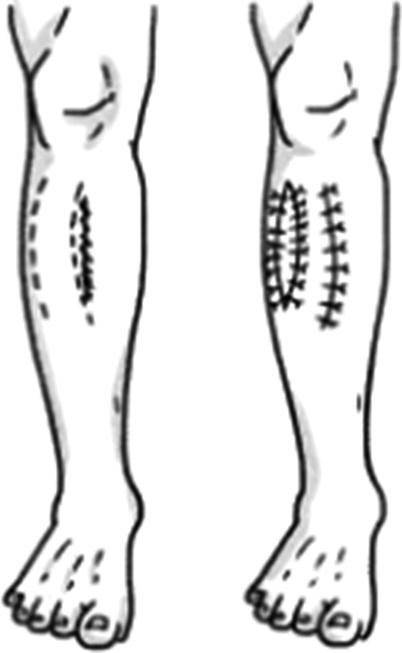
Fig. 3.10
Sliding skin flap. (a) Design of sliding advancement skin flap. (b) The sliding skin flap is advanced to repair the wound. (c) Suture
Fig. 3.11
Double-pedicle gliding skin flap
- 1.
Design: At one side or both sides of the defect wound, according to the need of repair, the skin flaps can be designed as tonguelike, rectangular, and triangular and can be designed as single or double skin flaps. When a double-pedicle skin flap is designed, the length-to-width ratio of the skin flap can be doubly increased (3:1). The methylrosanilinium chloride is used to mark out the incision line.
- 2.
Transfer: The skin and subcutaneous tissue are incised open along the designed incision line. The skin flap is dissociated from the distal end of the skin flap (at the superficial surface of the deep fascia) to the pedicle, and it is advanced through gliding after adequate dissociation and is transplanted to cover the wound in the receptor site. In general, no secondary wound will appear in the donor site of single-pedicle skin flap, but the skin wrinkles will often be formed at both sides of the pedicle. The smaller wrinkles will disappear themselves in the future; otherwise, a piece of triangular skin tissue is removed in the place where skin wrinkles exist, so as to flatten the skin wrinkles and heal the wound; if it is estimated that the removal of this triangular skin tissue may affect the blood supply of the skin blood supply, this triangular skin tissue should be retained to be removed in the two-stage operation. The donor site where the double-pedicle skin flap is formed often cannot be sutured without tension; otherwise, the secondary skin defect wound will appear, which needs to be repaired through harvesting the split-thickness skin.
2.8.2 Rotation Skin Flap
The rotation skin flap is the skin flap formed in the adjacent site of the defect wound, and it is used to repair the defect through rotational transplantation. This kind of skin flap is flexible and changeable compared with the advancement skin flap and is widely used.
- 1.
Design
- (a)
Tongue-shaped skin flap: The skin flaps are generally designed to be tongue-shaped. According to the shapes and sizes of the skin defect wounds, following the principles of skin flap design, the skin flaps are designed at one or both sides of the defect wounds, and the methylrosanilinium chloride is used to mark them (Fig. 3.12). When the skin flap is designed, attention should be paid to that the distance between the rotation pivot point of the skin flap and the farthest point of the skin flap must be greater than or equal to the distance between the rotation pivot point of the skin flap and the farthest point of the defect wound margin; otherwise, the skin flap will not be able to cover the entire defect wound, even if the entire defect wound is covered with an effort. The blood supply will be affected due to excessive tension, when the donor site of the rotation skin flap is located in the functional site or exposed site and because the wound is larger and cannot be directly sutured. If the wound is repaired with skin graft, it may be possible to affect the function or morphology. Therefore, a smaller skin flap is redesigned in the adjacent area of the wound, which is rotated to repair the wound in the donor site of the first skin flap. In general, the wound in the donor site of the smaller skin flap can be directly sutured. When the pedicles of the two skin flaps are located in the adjacent areas, they can be connected into a pedicle. This kind of skin flap is called the bilobed skin flap (Fig. 3.13).
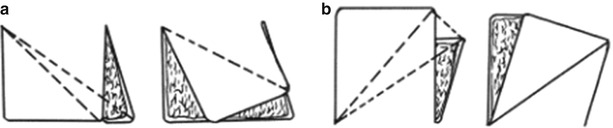
Fig. 3.12
Design of rotation skin flap. (a) The design of rotation skin flap is incorrect, resulting in tension. (b) The design of rotation skin flap is correct
Fig. 3.13
Bilobed skin flap
- (b)
Rhomboid skin flap: If the defect wound in receptor site is rhomboid-shaped, the skin flap can be designed as the rhomboid-shaped skin flap for transfer repair or designed as the polygonal (similar to rhomboid-shaped) skin flap for repair. This skin flap is most appropriately designed in the cervical area, and it has certain advantages for transfer repair of the rectangular defects in the lower face. The design of rhomboid skin flap is shown in Fig. 3.14, wherein abcd are rhomboid-shaped defects. The extension line of bd is made as de, ensuring that de = ab; then the parallel line ef starting from the e is made parallel to dc, and de and ab are sutured with each other after transfer.
Fig. 3.14
Design of rhomboid skin flap
- (a)
- 2.
Harvesting and transfer
- (a)
Tongue-shaped skin flap: The skin and subcutaneous tissue are incised open along the designed incision line. The dissociation is performed at the superficial surface of the deep fascia from the distal end of the skin flap to the pedicle, and the skin flap is completely lifted, and then the skin flap is rotated and transferred to repair the wound. In order to avoid excessive distortion after the transfer, a small piece of triangular skin tissue on the outside of the pedicle can be removed.
- (b)
Bilobed skin flap: After the first skin flap is harvested and transferred, the skin flap is incised, harvested, and transferred, and then the donor site of the second skin flap is repaired, and the donor site of the second skin flap is directly sutured.
- (c)
Rhomboid skin flap: Incise the skin along the design line, deep up to the superficial surface of the deep fascia; dissociate along the superficial surface of the deep fascia. It is noted that the dissociation scope should be larger, and thus the skin flap after transfer can be sutured without tension.
- (a)
2.8.3 Subcutaneous Pedicle Skin Flap
Subcutaneous pedicle skin flap is an advancement skin flap, namely, the edge of the skin flap is completely incised open, then the subcutaneous tissue of the skin flap is taken as the pedicle, and using its looseness, the skin flap is slid and transferred to repair the defects, which is commonly used in the repair of skin tissue defects in fingertips (Fig. 3.15) and has advantages that the operation is simple and the incision heals smoothly. But the subcutaneous tissue pedicle of such skin flap has no well-known artery and is not similar to the island skin flap; thus, the advancement distance is limited.
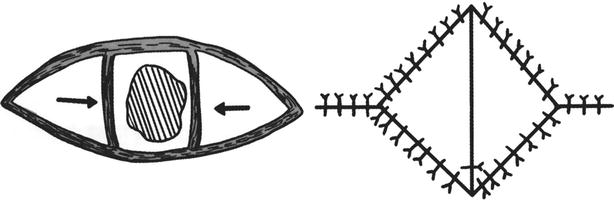
Fig. 3.15
Design and suture of bilateral advancement subcutaneous pedicle skin flap
- 1.
Design: According to the need of repair in the donor site, the skin flaps can be designed as triangular, round, rectangular, or polygonal skin flaps. Since the advancement distance of the skin flap is limited, the skin flaps are often designed to be located in the adjacent areas of the defects. If the skin flap formed in the adjacent area on one side of the defect is not sufficient to repair the defect, multiple subcutaneous pedicle skin flaps can be formed simultaneously in the adjacent areas on two or three sides of the defect, and then they are glided and transferred to repair the defect.
- 2.
Transfer: The skin and subcutaneous tissues are incised open along the marked incision line, directly down to the deep fascia, but they are not dissociated. The skin flap is slid and advanced into the defect area to cover the wound. The areas around the skin flap are sutured directly after a short separation; if it is difficult to perform a direct suture, the repair can be performed through transfer of the skin flap formed at its adjacent areas.
2.9 Distal Skin Flap Transplantation
When it is inappropriate or impossible to harvest the skin flap in adjacent areas of the defect, the skin flap far away from defect area is transferred into the donor site to repair the defect, which is called the distal skin flap transplantation. The skin flap is transferred directly from the donor site into the receptor site, which is known as distal skin flap transplantation; if the skin flap needs to be transited in the intermediate station and then is transferred into the receptor site, it is known as indirect distal skin flap transplantation. If the donor site is located in the limb of one side, and the formed skin flap is transferred to repair the tissue defects in the limb of the other side, it is called as the cross-skin flap transplantation. More than two operations are often required to complete the whole process of the distal skin flap transplantation.
2.9.1 Direct Distal Skin Flap
- 1.
Design: The repair of the tissue defect in the forearm with the abdominal skin flap is taken as an example. A piece of paper is sheared into a figure of the skin flap with an area slightly larger than the defect wound according to the shape of the defect. The paper figure of the skin flap is fixed onto the defect area in the forearm, and then the paper figure carried by the forearm is transferred and placed into the abdomen (Fig. 3.16); the specific location is appropriate if the patient feels more comfortable, and it is estimated that the pedicle will not be unduly distorted in the process of skin flap transfer. Then the pedicle of the paper figure is fixed onto the abdomen; after that, the forearm is moved away, and the paper figure will be flattened; the abdominal skin flap is drawn up according to the paper figure.
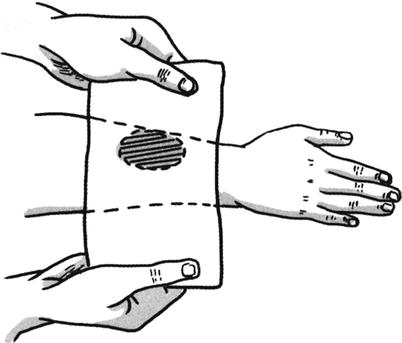
Fig. 3.16
Design of distal skin flap
- 2.
Transfer: The skin tissues are incised open along the design line of the skin flap, which is lifted from the superficial surface of the deep fascia. The flap area is transplanted into the receptor site, and the wound margin of the skin flap is interruptedly sutured with the wound margin of the receptor site (Figs. 3.17, 3.18, and 3.19). The pedicle is still connected to the donor site to ensure that the skin flap can get the blood supply from the donor site, namely, before the flap area of the skin flap establishes sufficient blood circulation; the skin flap can maintain its nutritional metabolism based on the blood supply of the pedicle. The secondary wound in the donor site after harvesting of the skin flap is treated depending on the size of the skin flap; if the wound is smaller, it can be directly sutured; if the wound is larger and cannot be sutured, it will be repaired with the harvested split-thickness skin graft. A sufficient blood circulation can be established between the flap area and the donor site at 2–3 weeks after surgery; after the vascular occlusion test confirmed that the blood circulation can maintain the metabolism of the skin flap, the pedicle separation can be carried out. The pedicle is cut off; the skin flap and the incision in the donor site of the forearm are sutured, respectively; and the skin flap transfer operation is completed. At the moment, in general, the wound in the donor site is directly sutured.

Fig. 3.17
Design of distal skin flap (1)

Fig. 3.18
Design of distal skin flap (2)
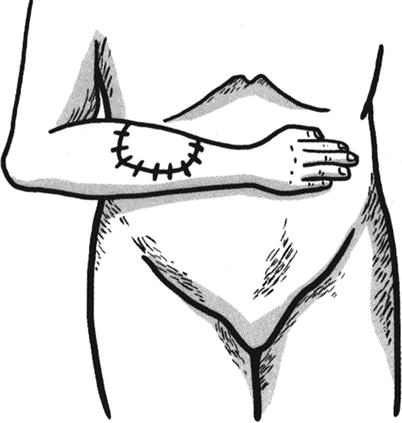
Fig. 3.19
Design of distal skin flap (3)
2.9.2 Indirect Distal Skin Flap
The indirect distal skin flap refers to the distal skin flap needing transition in the intermediate station. After the skin flap is formed from the donor site, the pedicle of the skin flap is transplanted into the intermediate station, after the blood supply which can maintain the metabolism of the skin flap is established between the skin flap and the intermediate station, and then the skin flap carried by the intermediate station is transplanted to the receptor site. At about 3 weeks after surgery, the sufficient blood supply has been established between the skin flap and receptor site, and then the pedicle of the skin flap is cut off from the intermediate station. More than three operations at least are required to complete the whole process of the distal skin flap transplantation.
- 1.
Design: The intermediate stations are usually designed and placed in the wrist or forearm. The skin flaps are designed according to the reverse design method, and the repair of tissue defects in the right temporal area with the abdominal skin flap is taken as an example. According to the size and shape of the temporal defect, a paper figure with an area slightly larger than the defect wound is sheared, and then the paper figure is used to cover the right temporal defect area. The left forearm (intermediate station) is transferred into the right temporal area, and the pedicle of the paper figure of the flap is fixed in the forearm and is marked; the paper figure carried by the forearm is transferred to the abdomen; then the paper figure is fixed in the abdomen; after the paper figure is flattened, the methylrosanilinium chloride is used to mark it. The specific locations of the abdominal skin flap and its pedicle are appropriate if the patient feels more comfortable, and the pedicle will not be unduly distorted in the transfer process.
- 2.
Implementing the harvesting and transfer surgery by stage.
- (a)
The first-stage operation: According to the design, the pedicle of the skin flap is incised open and harvested. The broken end wound of the pedicle is used to print a blood marker in the marked area on the left forearm, and a skin flap which turns to the medial side is formed along the size of the blood marker. The forearm is transferred to the abdomen, and then the pedicle of the abdominal skin flap is sutured with the forearm wound and the reversed skin flap. When the suture is performed, it is noted that 1–2 needles of mattress sutures are performed at the centers of the pedicle and the forearm wound to prevent the formation of dead space. The forearm and abdomen are properly fixed after surgery.
- (b)
The second-stage operation: At 2–3 weeks after the previous operation, the pedicle of the skin flap has been integrated with the intermediate station (left forearm) and healed; after the vascular occlusion test confirms that the blood supply from the pedicle can maintain the metabolism of the skin flap, the second-stage operation can be carried out. The abdominal skin flap is incised open and harvested, which is carried by the forearm (intermediate station) and transferred to the temporal defect area. The wound margins on the both sides of a segment of skin flap which is close to the pedicle are usually sutured with each other, so that there is no exposed wound in the pedicle, and the chance of postoperative secondary infection is reduced in the skin flap after operation. The forearm is fixed with the head after operation.
- (c)
The third-stage operation: At 2–3 weeks after the second-stage operation, good blood circulation has been established between the skin flap and temporal area (donor site), which is confirmed by the vascular occlusion test, and then the third-stage operation can be carried out. The pedicle attached to the intermediate station is cut off, and then the temporal defect area is repaired. The forearm skin flap lifted in the first-stage operation is sutured back into the previous place after the removal of the scar tissue.
- (a)
After the first- and the second-stage operations, it is very important that the limb taken as the intermediate station must be properly fixed with the abdomen and the donor site to prevent the skin flap avulsion (Figs. 3.20, 3.21, 3.22, 3.23, and 3.24).

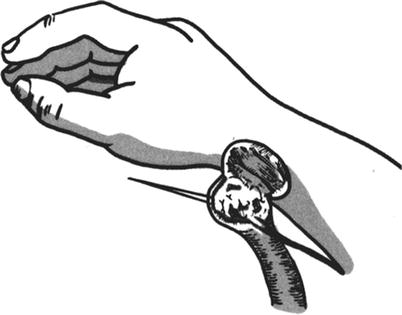
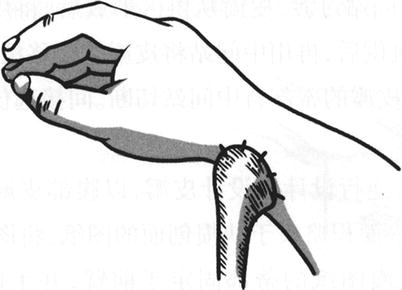
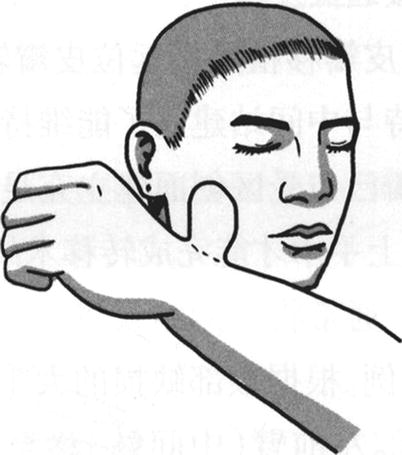
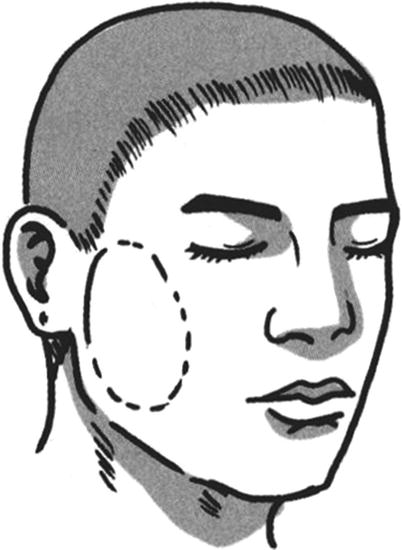
Fig. 3.20
The formation of the forearm wound (intermediate station) and the fixed suture of the pedicle of skin flap (1)
Fig. 3.21
The formation of the forearm wound (intermediate station) and the fixed suture of the pedicle of skin flap (2)
Fig. 3.22
The formation of the forearm wound (intermediate station) and the fixed suture of the pedicle of skin flap (3)
Fig. 3.23
The formation of the forearm wound (intermediate station) and the fixed suture of the pedicle of skin flap (4)
Fig. 3.24
The situation after repair of facial defect with forearm skin tube
3 Tubular Skin Flap
The wound margins on both sides of the skin flap are sutured with each other to form into a tubular skin flap in the process of the formation and transfer; hence, this kind of skin flap is named as the tubular skin flap (skin tube for short) (Fig. 3.25). Correspondingly, the skin flaps whose lateral sides are not sutured with each other, with a flat shape, are collectively called the flat skin flap. Compared with the flat skin flap, the skin tube has the main advantages that no wound is exposed in the transfer process, and the chances of infection are greatly reduced; and its disadvantages are that multiple operations are required to complete the whole transfer process. The scar formation is increased once along with that every operation is performed, and more skin tissues are lost in the process of completing the transfer.
Fig. 3.25
The sites where the skin tubes are prepared
3.1 Skin Tube Design
An elongated skin flap is designed in the donor site; because the skin flap has two pedicles, the length-to-width ratio is generally 2.5–3:1; if the donor site is located in the site with a good blood supply, the length-to-width ratio can be enlarged to 5:1. If the desired length-to-width ratio exceeds the ratio limit due to the need of repair, 1–2 pedicles (called “bridge”) can be added to the middle part of the skin tube (Figs. 3.26, 3.27, 3.28, 3.29, and 3.30). There are more operations in the process of skin tube transfer; the higher the number of operation is, the more the loss of skin tissue is. Therefore, in general, the design area of the skin tube should be greater than the wound area in the donor site by 30%.
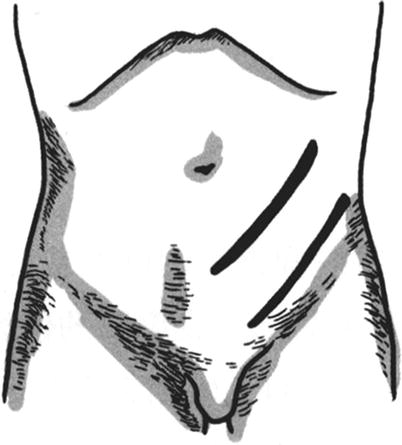

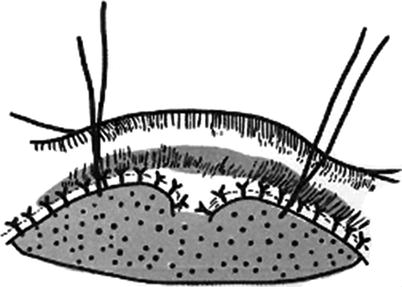

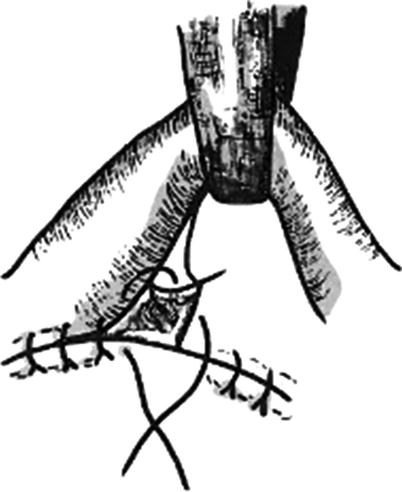
Fig. 3.26
Skin tube formation (1)
Fig. 3.27
The “bridge” in the middle part of the skin tube (1)
Fig. 3.28
The “bridge” in the middle part of the skin tube (2)
Fig. 3.29
Skin tube formation (2)
Fig. 3.30
Skin tube formation (3)
The elongated skin flaps are not necessarily designed as rectangular skin flaps. They can be designed into the S-shaped and C-shaped skin flaps (Fig. 3.31), in order to increase the actual length of the skin tube.
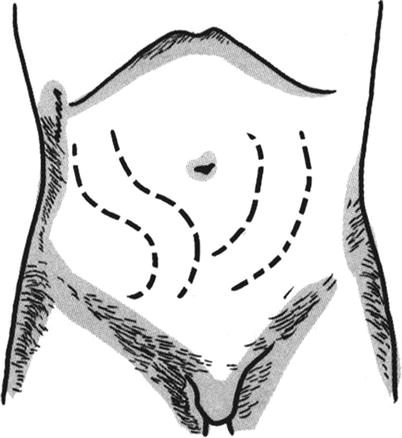
Fig. 3.31
Formation of S-shaped and C-shaped skin tubes
3.2 Skin Tube Formation
The skin and subcutaneous fat on one side of the elongated skin flap are incised open according to the designed incision line. The dissociation is performed along the superficial surface of the deep fascia, directly reaching to the incision line on the other side of the skin flap. It is noted that a triangular-shaped area of subcutaneous tissue is reserved, respectively, in the pedicles at the both ends of skin flap (Fig. 3.32) when the dissociation is performed, so as to prevent emergence of the dead spaces in the pedicles after skin tube is sutured. It is experimented that the skin flap edge which has been dissociated is rolled to the incision line in the other side which has not been dissociated. It is estimated that the skin flap after being sutured into the skin tube has neither tension nor dead space, and then the incision line on this side is incised. Otherwise, the location of the incision line on one side which is not incised open is adjusted to change the width of the elongated skin flap, and then the skin and subcutaneous fat is incised open along the adjusted drawing line. After careful hemostasis, the skin flap is sutured into the skin tube with the full-thickness interrupted suture (Fig. 3.33). If the secondary wound in the donor site where the skin tube is formed can be directly sutured, the wound in the connecting area between the two pedicles of the skin tube and the donor site should be sutured by means of a mattress suture (Fig. 3.34), so that the wound is completely closed; if the secondary wound cannot be directly sutured, the split-thickness skin graft will be additionally harvested and transferred to repair the wound (Fig. 3.35). After the formation of the skin tube and before carrying out bandaging, a gauze roll which has the same size of the skin tube and is slightly longer than the skin tube is placed, respectively, on both sides of the skin tube to prevent the skin tube compression (Fig. 3.36), and both ends of the gauze roll are fixed onto the skin in the donor site, respectively, with a stitch.
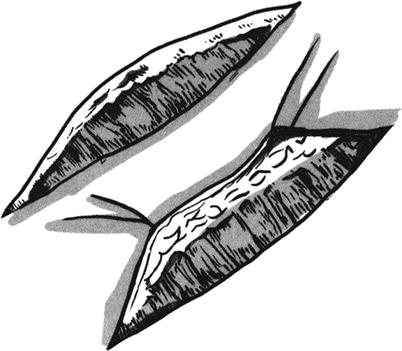
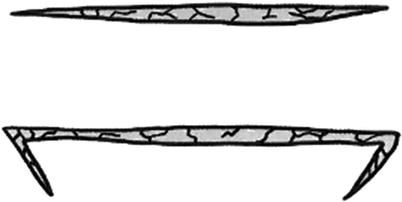

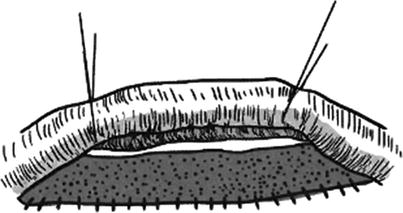
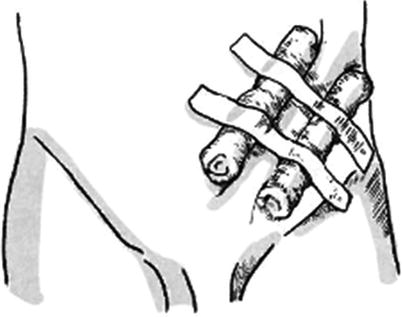
Fig. 3.32
Skin tube formation
Fig. 3.33
Unilateral additional incision suture (1)
Fig. 3.34
Unilateral additional incision suture (2)
Fig. 3.35
The skin graft is used for the donor site under the skin tube
Fig. 3.36
The bandaging method for the formed skin flap
3.3 Skin Tube Transfer
The skin tube can be transferred at 3 weeks after formation. The skin tube transfer includes two methods such as direct transfer and indirect transfer.
3.3.1 Direct Skin Tube Transfer
The skin tube transfer can be performed at 3 weeks after the formation of the skin tube, after the vascular occlusion test suggests that the blood supply of the pedicle of the skin tube is good enough to maintain the nutritional metabolism of the whole skin tube. The end where the vascular occlusion test is performed is cut off from the donor site; if the broken end has no active bleeding or the skin tube is pale, it indicates poor blood supply; thus, the broken end of the skin tube should be sutured back into its original place. After 3 weeks, the vascular occlusion test and skin tube transfer are carried out again; if the broken end has active bleeding, it indicates good blood supply, and then the transfer can be carried out. According to the need of repair, at first, the skin tube is cut open along the suture scar, and the scar tissue is removed; finally the skin tube is flattened and transplanted to repair the defect in the receptor site, and finally, the wound margin is sutured interruptedly. The pedicle is cut off at 2–3 weeks later. The pedicle of skin tube is cut and trimmed, and the wounds in the donor site and the receptor site are sutured, respectively.
3.3.2 Indirect Skin Tube Transfer
The indirect skin tube transfer is similar to the indirect method for flat skin flap transfer. The intermediate station must be as a transition in the indirect skin tube transfer, and the wrist is usually taken as the intermediate station. At 3 weeks after the formation of the skin tube, the vascular occlusion trials suggest good blood supply in the pedicle; thus, the first-stage transfer is performed. The pedicle of the skin tube is cut off and is transferred to the intermediate station (see Figs. 3.20, 3.21, 3.22, 3.23, and 3.24). After its establishment of good blood supply with the intermediate station, the second-stage transfer is performed. The pedicle at the other end of the skin tube is cut off, so that the skin tube is completely separated from the donor site, and then is incised open to form into a skin flap. At last, the skin tube carried by the intermediate station is transferred to repair the defect in the receptor site. After a good blood supply has been established between the skin flap and the donor site at 2–3 weeks later, the pedicle is cut off to complete the whole process of transplantation. Before each transfer operation is performed, it is required to carry out vascular occlusion test.
There are two commonly used methods for the vascular occlusion test:
- 1.
The color agent which is not easy to fade or 10% silver nitrate is used to mark the area where it is to be cut off during the time of transfer. The rubber strip is used to bypass the skin tube along the marked line, and then is fastened and tightened until that the blood flow is completely blocked. If there is no change in the color of the skin tube at 1 h after the rubber strip is fastened, it suggests that the pedicle at the other end of the skin tube has been able to provide good blood circulation.
- 2.
The sphygmomanometer pneumatic cuff is used to fasten the limb which carries the skin tube at the proximal side of the intermediate station, the sphygmomanometer is inflated until the pressure is higher than the arterial pressure (systolic pressure). If the distal end of the fastened limb has already felt numb and cold, and there is no change in skin color of the skin tube, and the skin temperature is normal, it suggests that the skin tube has a good blood supply, and its connection to the intermediate station can be cut off.
The vascular occlusion test can also be used for training of the skin tube blood supply; at 2–3 weeks after the formation of the skin tube, the blood flow is blocked for 2–3 min on the first day, once a day; the time of blocking the blood flow is extended day by day until the skin tube has a good blood supply.
One or more “bridges” can be designed in the middle segment of the ultralong skin tube, namely, every “bridge” is a pedicle, thus increasing the blood supply to the skin tube. During the skin tube transfer, the “bridge” should be cut off at first; the treatments before and after surgery are the same as those of cutting off the pedicle, namely, it is needed to perform the vascular occlusion test before surgery, and the next stage of the operation can only be carried out at 2–3 weeks after surgery.
4 Axial Pattern Skin Flap
The axial pattern skin flap is also known as the arterial skin flap. It is the skin flap which is designed through taking the well-known artery as the axial artery. The entire skin flap is provided with blood by the axial artery; thus, the skin flap is not limited by the traditional length-to-width ratio, and the scope of the infusion of the axial artery is taken as the maximum area of the skin flap. In order to expand the area of the skin flap, a random pattern skin flap can be carried at the distal end of the axial pattern skin flap.
The existence of the axial artery is a prerequisite for the formation of axial pattern skin flap, which is also the dominant factor to determine the characteristic of the axial pattern skin flap; therefore, the axial pattern skin flap should be named according to the axial artery which constitutes the skin flap. The random pattern skin flap can be named after the place where it is located, such as chest skin flap and abdominal skin flap. It can also be named according to its shape, such as leaf skin flap, triangular skin flap, and tubular skin flap. These names can sufficiently show the properties of the skin flaps. For the naming of the axial pattern skin flap, the axial artery should be included in the name of each skin flap to show its characteristics, and it also can avoid the occurrence of the confusing phenomenon of different skin flaps having the same name or the same skin flap having multiple names. For example, in term of the forearm axial pattern skin flap, if the radial artery is taken as the axial artery, it should be named as the radial artery forearm skin flap; if the ulnar artery is taken as the axial artery, it should be named as the ulnar artery forearm skin flap. For another example, the posterior tibial artery can be taken as the axial artery of the axial pattern skin flap in the anteromedial calf, and the cutaneous branch of the tibial nutrient artery can also be selectively used as the axial artery; the selectively used axial blood vessels are different; the characteristics of the skin flaps are different. The skin flap taking the posterior tibial artery as the vascular pedicle should be referred to as the posterior tibial arterial skin flap in the anteromedial calf. Because this skin flap has large-caliber blood vessels, the vascular anastomosis operation is easy with a high success rate, but it requires the sacrifice of a main artery in the calf, and it should be considered as the contraindication in the patients with anterior tibial artery dysfunction. The skin flap in the anteromedial calf takes the cutaneous branch of the tibial nutrient artery as the vascular pedicle, it is thin and its texture is fine, it does not require the sacrifice of a main artery in the calf, and the wound in the donor site is small, but the vascular caliber is not as thick as that of the tibial artery, with higher technical requirements for anastomosis. It should be referred to as the skin flap in the anteromedial calf with the cutaneous branch of the tibial nutrient artery, in order to be differentiated from the skin flap in the anteromedial calf with the posterior tibial artery. It is not rare that a skin flap has two or more than two names, for example, in terms of the perineum axial pattern skin flaps which take the posterior artery of the labia (scrotum) as the axial arteries, some are called as the perineum axial pattern skin flaps, and some are also called as the pudendal thigh skin flaps. If the axial artery is marked in its name, not only will the characteristics of the skin flap be clear at a glance but also will the name confusion be avoided.
4.1 Classification of Axial Pattern Skin Flaps
- 1.
Peninsula axial pattern skin flap: The peninsula axial pattern skin flap is usually called the pedicled axial pattern skin flap. In the process of transplantation, in addition to the axial blood vessel, the skin and subcutaneous tissue in the pedicle are also connected with the donor site. This kind of skin flap is transferred into the donor site by means of pedicled transfer, and the specific operation is similar to the local transplantation of the random pattern skin flap.
- 2.
Island skin flap: In the process of island skin flap transplantation, only the axial blood vessel bundle of skin flap in the pedicle is connected to the donor site. After the formation of the skin flap, the skin in the proximal end of the pedicle is incised open to isolate the axial blood vessel bundle, and the island skin flap is transferred into the receptor site usually through subcutaneous tunnel or incising open the normal skin tissue between the donor site and the receptor site. When the vascular pedicle is being isolated, it is needed to retain a little loose connective tissue to prevent damage to blood vessels. In the process of the transfer, the width of the subcutaneous tunnel should be sufficient to prevent the vascular bundle compression.
- 3.
Free skin flap: In the process of transplantation, the axial artery and vein are cut off; the skin flap is completely separated from its donor site. The artery and vein in the vascular pedicle of the skin flap are anastomosed, respectively, with those in the receptor site with the small vascular anastomosis technique, so that the skin flap can get the blood supply immediately from the donor site.
4.2 The Advantages of Axial Pattern Skin Flap
- 1.
The blood supply of the axial pattern skin flap is rich and has a strong resistance to infection; therefore, it can be used for repair of contaminated skin tissue defects or skin tissue defects with poor blood supply
- 2.
The area of the axial pattern skin flap is not restricted by the length-to-width ratio. The skin flap can be formed within the scope of perfusion of the axial artery, and thus, it is designed flexibly and can meet the need of repair of skin defects of different shapes.
- 3.
When the distal axial pattern skin flap is transferred, the axial blood vessel bundle of skin flap can be anastomosed, respectively, with the arteries and veins in the receptor site. The whole process of the skin flap transfer can be completed in an operation, which can reduce the pain of the patient and shorten the hospital time.
- 4.
According to the need of defect repair in donor site, the pedicles of the axial arteries and veins of two or more skin flaps can be anastomosed with each other to form into the common vascular pedicle shared by multiple skin flaps, and then the axial arteries and veins of this vascular pedicle are anastomosed, respectively, with those in the receptor site, so that the multiple skin flaps are transplanted by means of series or parallel connection.
4.3 Commonly Used Axial Pattern Skin Flaps
The pedicled or free transplantation of commonly used axial pattern skin flaps for repairs is shown in Table 3.2.
Table 3.2
Pedicled or free transplantation of commonly used axial pattern skin flaps for repairs
Names of skin flaps | Main axial pattern blood vessels | Repair sites |
|---|---|---|
Parietal skin flap | The parietal branch of superficial temporal artery | Scalp, beard, and eyebrow defect |
Forehead skin flap | The frontal branch of superficial temporal artery | Face, organ defects, oral perforating tissue defect |
Temporal skin flap | Superficial temporal artery | Face, ear, nasal, and orbital reconstructions, free transplantation for repair of hand soft tissue defect, and joint exposure |
Postauricular skin flap | Posterior auricular artery and superficial temporal artery – posterior auricular artery | Forehead, the area around the eye, nose, face, or free transplantation |
Deltopectoral skin flap | The perforating branch of internal thoracic artery | Jaw and neck |
Lateral thoracic skin flap | Lateral thoracic artery | Armpit, chest wall |
Lateral thoracoabdominal skin flap | Lateral cutaneous branch of the intercostal artery | Breast reconstruction, thoracic dorsal areas, contralateral forearm |
Paraumbilical skin flap | Paraumbilical branch of the inferior epigastric artery | Contralateral thoracoabdominal wall, contralateral forearm and hand or free transplantation |
The iliolumbar skin flap | Superficial epigastric artery, superficial iliac circumflex artery | Forearm, hand, perineum, great trochanter, or free transplantation |
Scapular skin flap | Circumflex scapular artery | Shoulder, armpit, upper arm or free transplantation |
Medial arm skin flap | Superior ulnar collateral artery | Maxillofacial and cervical regions, shoulder, elbow, or free transplantation |
Lateral arm skin flap | Radial collateral artery | Shoulder, axilla, elbow, or free transplantation |
Forearm (radial artery) skin flap | Radial artery | Hand (retrograde transfer) or free transplantation |
Dorsal skin flap of index finger | The first dorsal metacarpal artery | Thumb, thumb web |
Anterolateral thigh skin flap | The descending branch of femoral anterolateral artery | Groin, perineum, greater trochanter, descend retrograde to the knee, upper pretibial region or free transplantation |
Medial femoral skin flap | The cutaneous branches of the femoral artery | Free transplantation for repair of soft tissue defects in sites such as planta pedis and hand |
Saphenous arterial skin flap | Saphenous artery | Pretibial area, knee, forearm, hand, and palm |
The medial crural skin flap | Posterior tibial artery | Knee, upper crus, ankle, palm, or free transplantation |
The lateral crural skin flap | Peroneal artery | Knee, pretibial area, lower crus, ankle, or free transplantation |
Dorsalis pedis skin flap | Dorsal pedal artery | Ankle, heel, pretibial area |
Medial plantar skin flap | Medial plantar artery | Heel, ankle, palm of the hand, thumb web |
5 Free Skin Flap
5.1 Overview
The skin flap consists of the skin and subcutaneous tissues with blood supply. The part of the skin flap connected with the body is known as the pedicle, which is the blood supply source of the skin flap after transfer. When the skin flap is being harvested, the pedicle is composed of the skin, subcutaneous tissues, fascias, muscles, or blood vessels which are not completely cut off. After the skin flap is completely cut off, the vascular anastomosis is performed with the microsurgical techniques to re-establish the blood supply, and this kind of skin flap is called the free skin flap. The area providing the tissue structure of the skin flap is called the donor site of the skin flap; the area repaired and covered by the skin flap is called the receptor site of the skin flap. In the early stage of skin flap transfer, its blood supply and nutrition depend entirely on the pedicle. In the late stage, the blood supply of the skin flap can also be obtained from the tissues in the bottom of the receptor site and the surrounding areas.
The free skin flap transfer or transplantation began in 1972 and is currently the most important treatment means in plastic surgery. The free skin flap transplantation technique greatly facilitates the developments of plastic surgery, orthopedics, trauma surgery, hand surgery, and other related professions, and it is a major innovation for surgical techniques in the second half of the twentieth century. The free skin flap transplantation with vascular anastomosis has characteristics such as flexible skin flap design, diverse tissue constituents, random size and rich blood supply, and less number of operations. The free skin flap transplantation can be used in the early and late surgical repairs of severe traumas to preserve limbs, reduce amputations, and maximize the functional recovery; it can make the one-stage repair of body surface tumor resection possible; it can meet the needs of repairs of different tissue and organ defects in trauma surgery and oncological surgery; it can maximally guarantee complete removal of the lesions to protect and reconstruct the tissues and vital organs and to obtain a satisfactory appearance. The pedicled skin flap has irreplaceable advantages for some patient cases. But the free skin flap transplantation requires skilled microsurgical techniques, which has disadvantages such as longer operative time, needing more staff and certain equipments and complex technical operations. Indeed the free skin flap transplantation has certain risks and failure rates.
The general and local conditions; vascular conditions, especially the blood circulation statuses such as the blood vessel diameter, location, and distance; and the healthy conditions of the blood vessels themselves and their surrounding tissues in the patients should be carefully examined and objectively evaluated before free skin flap transplantation. The patency and directions of the pedicle blood vessels and the vascular conditions in the receptor sites should be routinely detected with Doppler blood flowmeter before surgery, and the directions of the blood vessels in the body surfaces of patients are marked with methylene blue. If necessary, the computer tomography angiography is performed to reduce the blindness of operation.
Related posts:
 Microcirculation Model for Invasive Animal Monitoring
Microcirculation Model for Invasive Animal Monitoring
 Composite Osseomusculocutaneous Thymus Allotransplantation Model
Composite Osseomusculocutaneous Thymus Allotransplantation Model
 In Vivo Chimera Model: Creation of Primary and Secondary Chimera
In Vivo Chimera Model: Creation of Primary and Secondary Chimera
 Experimental Model for Monitoring of Composite Tissue Transplantation Induced Trauma
Experimental Model for Monitoring of Composite Tissue Transplantation Induced Trauma
 Neuroma Model
Neuroma Model
 Tissue Engineering and Oncological Surgery
Tissue Engineering and Oncological Surgery
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


