The alar cartilages provide the contour and structural support of the nasal tip. Current rhinoplasty concepts support preservation of alar structure with suture techniques or judicious cephalic trim indicated for tip deformities. In many primary cases and some revisions, adequate alar structure exists to achieve the desired aesthetic and functional results with conservative surgical methods. In some primary and most revision cases, however, the existing tip structure is inadequate to create a structurally sound and aesthetically pleasing nasal tip without adding structure. In these cases, alar cartilage grafting techniques are indicated to recapitulate nasal tip contour and structure.
The initial approach to rhinoplasty begins with complete nasal and facial analysis to fully characterize aesthetic and structural problems. Only then can a surgical plan be created that may or may not involve alar cartilage grafting.
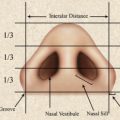
The face can be divided into equal vertical fifths. There is a single region between the medial canthi and paired regions between the lateral aspect of the pinna and lateral canthus as well as paired regions between the lateral and medial canthi. The width of the nasal base should approximate the intercanthal distance and is approximately one fifth of the facial width. The vertical height of the face can be divided into horizontal thirds spanning the trichion to glabella, glabella to subnasale, and subnasale to menton. Thus, nasal length is ideally one third of facial height. Although these proportions are equal in the aesthetic ideal, the upper third of the face tends to elongate with age because of elevation of the hairline while the lower third contracts due to bony resorption of the mandible.
Analysis of the nasal tip
The alar cartilages provide the contour and structural support of the nasal tip. Current rhinoplasty concepts support preservation of alar structure with suture techniques ; judicious cephalic trim is indicated for tip deformities.
Tip Projection
Multiple methods exist to determine optimal nasal tip projection. These methods often provide different estimations of the aesthetic ideal. Thus, there is no single tool that provides the optimal measure of tip projection. Well-known methods include those of Goode, Simons, and Crumley. In brief, Goode’s method predicts an ideal ratio of 0.55 to 0.6 between the length of a line drawn from nasion to nasal tip relative to a perpendicular line from alar–facial sulcus to nasal tip. Crumley suggests that, ideally, the nose represents a 3-4-5 triangle. Lastly, Simons has estimated that the upper lip height (subnasale to vermilion) should approximate tip projection (subnasale to tip). The senior author uses the guideline of 10, 20, and 30 mm when assessing projection of the nasal dorsal line. Ideally, the nasion should project 10 mm anterior to the corneal plane. The rhinion and tip-defining point should project 20 and 30 mm, respectively, from the anterior facial plane, defined by a vertical line tangent to the alar–facial sulcus and nasion.
Tip Rotation
Ideal nasal tip rotation has been described in the literature. A frequently used correlate of tip rotation is the nasolabial angle. As a general rule, tip rotation in the male is a relatively acute, 90° to 105° nasolabial angle, while that in females is more obtuse, 100° to 120°.
Photographic documentation
While both film and digital photographic systems are available, most surgeons have transitioned to the digital format. This provides for rapid acquisition, processing, and printing of images. Further, current 35 mm digital systems provide excellent image quality. Typical views included in rhinoplasty photography include a frontal projection, base view, and lateral and oblique images. Some surgeons routinely include smiling lateral views to better assess dynamic tip movement with facial animation. It is critical that all lateral and oblique images are acquired in the Frankfort horizontal plane (a line connecting the superior aspect of the tragus to the infraorbital rim should be parallel to the horizontal), which allows precise comparison between pre- and postoperative images.
Photographic documentation
While both film and digital photographic systems are available, most surgeons have transitioned to the digital format. This provides for rapid acquisition, processing, and printing of images. Further, current 35 mm digital systems provide excellent image quality. Typical views included in rhinoplasty photography include a frontal projection, base view, and lateral and oblique images. Some surgeons routinely include smiling lateral views to better assess dynamic tip movement with facial animation. It is critical that all lateral and oblique images are acquired in the Frankfort horizontal plane (a line connecting the superior aspect of the tragus to the infraorbital rim should be parallel to the horizontal), which allows precise comparison between pre- and postoperative images.
Computer imaging
Although a discussion of computer imaging is beyond the scope of this article, this tool can provide an estimation of ideal postoperative results. Patients must be cautioned, however, that prediction of rhinoplasty results is fraught with difficulty and that modified images represent the ideal outcome rather than a guarantee. Please refer to the following source for discussion of the utility and accuracy of computerized imaging in prerhinoplasty consultation.
Sources of graft material
Autogenous cartilage harvested from the nasal septum, conchal bowl or rib is the ideal graft material ( Fig. 1 ). These grafts have very low risk of infection or extrusion compared with an alloplast. Cartilage grafts are tolerated well by nasal tissue and can be sculpted precisely to adapt to the recipient site. Scoring, morselization, or crushing of cartilage grafts also may be performed to create a more malleable graft material.
Nasal Septum
Septal cartilage represents the gold standard material for alar cartilage grafting. It can be accessed in the same operative field during rhinoplasty. The entire quadrangular cartilage with the exception of a 1 cm dorsal and caudal strut may be harvested without compromising dorsal or tip support ( Fig. 2 ). The available cartilage typically is robust, and beveling the edges of septal cartilage grafts can help soften their appearance and minimize their visibility and palpability. The occurrence of infection or extrusion is uncommon. The unoperated patient typically has a generous supply of septal cartilage. In cases of revision rhinoplasty, however, there is often inadequate cartilage available to the surgeon for required alar cartilage grafts. Preoperative palpation of the septum with a cotton swab may reveal the extent of submucous resection in previously operated patients, alerting the surgeon to the potential need to access non-nasal cartilage donor sites.
Auricular Cartilage
The conchal bowl provides an easily accessible source of cartilage or composite graft material. While requiring a second operative site, it can be easily incorporated within the surgical field prepared during rhinoplasty. Both medial and lateral approaches can be used to harvest the entire concha cymba and cavum without compromising the appearance of the pinna or structure of the cartilaginous ear canal. The medial approach ( Fig. 3 ) places a scar on the postauricular portion of the pinna, which is well-hidden from the casual observer. Alternatively, the lateral approach, which places a scar on the antihelical fold, heals well with minimal scarring. The appearance of the pinna is unaltered by either approach as long as the structure of the antihelical fold cartilage is preserved.
When used in rhinoplasty, conchal cartilage has similarly low rates of infection and extrusion compared with septal cartilage. Crushing or morselization of conchal cartilage is more likely to cause fragmentation as conchal cartilage tends to be weaker than septal cartilage. As a result, the cartilage often must be folded or doubled-over to achieve adequate rigidity. Concha cymba has the disadvantage of being bowl-shaped, which can result in few straight segments of cartilage. The contour of the concha cymba, however, makes this an ideal graft for replacing the lateral crus or the entire alar cartilage. The most common complications of conchal cartilage harvest are auricular hematoma and perichondritis. Hematoma is prevented by quilting with transauricular sutures or using a bolster dressing at the time of wound closure ( Fig. 4 ). Perichondritis is evidenced by erythema, edema, and induration of the cartilage-bearing portions of the pinna (not the lobule) and is managed with antipseudomonal antibiotics.
Rib Graft
A generous amount of costal cartilage is available for grafts. The senior author prefers to harvest costal cartilage from the sixth rib, as this allows incision placement within the inframammary crease. If required, cartilage from the seventh rib can be harvested through the same incision. The perichondrium is removed in its entirety, followed by concentric carving of the graft in balanced cross-sections. Despite these maneuvers, the most consistent complication of costal cartilage grafts is the propensity for warping. Many surgeons carve the graft immediately after harvest and allow initial warping of the graft before implantation. Thus, the initial tendency of the graft to warp can be recognized and countered with additional contouring. It has been shown experimentally, however, that grafts continue to warp on a long-term basis. To counteract this risk, some authors place a Kirschner wire along the longitudinal axis of the costal cartilage graft if it is being used as a dorsal onlay graft or columella strut.
Costal cartilage harvest requires general anesthesia, adding to total operative time and expense. In addition, the elderly are poor candidates for rib grafting, as ossification can interfere with graft harvest and carving. Although there is a risk of pleural violation and pneumothorax, these complications are uncommon and can be recognized intraoperatively with the Valsalva maneuver. Through the same exposure for harvesting the rib graft, a red rubber catheter is placed in the chest to evacuate intrathoracic air. As long as the visceral pleura remains intact, a thoracostomy tube is unnecessary. Patients undergo a postoperative chest radiograph if the Valsalva maneuver suggests violation of the pleura and are routinely discharged on the same day of surgery unless a pneumothorax develops.
Irradiated Costal Cartilage
Cadaveric rib cartilage, which has been gamma-irradiated to minimize the risk of infection and tissue rejection, is readily available. A necessary point of discussion with the patient is the implantation of cadaveric tissue. Although rarely a point of major concern, some patients are not agreeable to cadaveric tissue grafts despite the low risk of transmission of infectious disease. Controversy exists as to the long-term survival of this homograft material, but some authors demonstrate predictable, robust long-term results in correction of saddle nose deformity. Further, the severity of warping of fresh and irradiated cadaveric rib appears to be comparable. Although there is justifiable concern of long-term resorption of irradiated costal cartilage grafts, there is evidence that replacement with fibrous tissue can maintain the aesthetic appearance.
Alloplast
Medpor
Medpor is comprised of high-density polyethylene. This biomaterial is highly compatible with human tissue and commercially available preshaped for various nasal graft applications. The pore size of roughly 100 μm allows fibrovascular tissue ingrowth. This helps reduce the risk of implant migration, extrusion, and infection. The porosity of the implant also may allow bacterial colonization and potential graft infection. Thus, many surgeons soak the implant in dilute Betadine or antibiotic solution before implantation. The main drawback of using Medpor is the risk of extrusion caused by infection or implant mobility. Implants may be difficult to excise because of the fibrovascular tissue ingrowth.
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


