The nasal base is often overlooked during the initial planning of rhinoplasty. Poor surgical planning or improper correction of alar base disharmonies can be irreversible and can have significant functional consequences. This article simplifies the recognition of common alar base disharmonies. The classification system is intended to facilitate choosing the best surgical technique to correct the alar base flaws.
Disharmony of the alar base structure with the rest of the nose is the most common imperfection encountered in secondary rhinoplasty in the senior author’s (BG) practice. The deformity is often seen in the original structure of the wide base, which was neglected during the initial nasal evaluation and surgical planning. The disharmony may also arise because of changes made to the adjacent nasal structures, such as an increase in alar flare after significant reduction of the tip projection. Reduction of the nasal base width should be undertaken when the interalar distance exceeds the intercanthal distance in the Caucasian patient. Ethnic variations may be handled differently.
Alar base surgery is an important component of the aesthetic rhinoplasty procedure. Robert Weir is credited with the first external alar wedge excision in 1892 to correct the alar flaring after reduction rhinoplasty. Others, such as Joseph and Milstein, modified the technique in 1931 in an attempt to avoid the external scar by including the internal excisions from the nostril base and vestibular floor. Techniques to avoid scarring during rhinoplasty have been developed, but the Weir external alar wedge excision is still in use. Most of the current written works contain some modifications in the approach to the alar base excision. There is also a description of the cinching sutures to approximate the alae and narrow the nasal base. The most recent technique for correcting the broad nasal base, particularly for patients with a vertically oriented alar axis, uses alar release via an incision at the ala-sill junction, release of the periosteal ligaments, and approximation of the dermis on both sides with sutures to medialize the nasal base.
Improper correction of these alar base abnormalities can have unfavorable aesthetic and functional consequences. Once the tissue is removed, it is much more difficult to correct. The alar base imperfections must be properly evaluated from the onset and surgical correction performed with precision to avoid the need for secondary corrective surgery. Common alar base flaws that are correctable include flaring of the alar rims, a wide nostril sill, and a combination of the two.
Anatomy and nasal analysis
An essential component of achieving a natural appearing and balanced rhinoplasty outcome is attention to the alar base. In an ideal aesthetic nose, there is a harmonious relationship between the nose and other facial features. Thorough visual analysis of the face combined with the method of soft-tissue cephalometric analysis using life-sized photographs of the face facilitates planning the aesthetic goals of the operation. The life-sized photographs allow precise measurement of the facial elements.
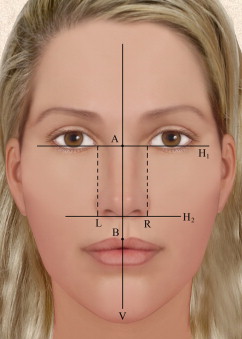
In the horizontal plane, the distance from one lateral alar base to the opposite one is approximately 2 mm wider than the intercanthal distance (ICD), the distance from one medial canthus to the opposite one. The ICD is usually 31 to 33 mm. If the ICD is abnormal, the distance of the orbital fissure (medial to lateral canthus) can be used as the reference. The ICD is bisected (point A) and a vertical line (line V) is drawn to pass the philtrum (point B) on an otherwise symmetric face. Two parallel lines (lines L and R) can then be symmetrically drawn in relation to the vertical midline, starting at the medial canthi and passing 1 mm medial to the outer boundary of the alar base ( Fig. 1 ). This is the Caucasian ideal, but ethnic differences and personal preference may deviate from this ideal.
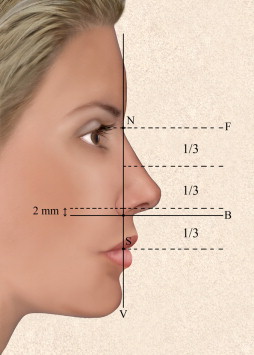
In the vertical dimension, best seen on the profile view, the caudal margins of the alar base are located approximately 2 mm cephalic to a line separating the middle two-thirds from the lower one-third of the distance from the medial canthus to the stomion. Point N (nasion) denotes the deepest portion of the ideal nasofrontal groove, or the level of the lower border of the upper lid margin on straight gaze, in those with a less-shallow or too-deep nasion. Point N is connected to point S (stomion), the junction of the upper and lower lips, by the vertical line V divided into 3 equal lengths ( Fig. 2 ).
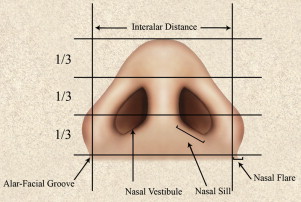
Evaluation of the base of the nose should also include the size, shape, and symmetry of the nostrils and the width and length of the columella and its relationship to the height of the lobule and the thickness and contour of the alae. The ideal nasal base resembles an equilateral triangle, with the length of the columella being twice the height of the infratip lobule ( Fig. 3 ). The nostrils should be oval-shaped, and should be wider than the columella. The long axis of the nostrils in a Caucasian should be oriented almost parallel to the vertical axis of the columella, with the anterior portion slightly narrower than the posterior portion. Ethnic variations can be seen in the shape and orientation of the nostrils. The character of the skin, either thick or thin, should also be noted and considered in choosing the type of alar base reduction.
Vertical plane alar base deformities
Disharmonies of the alar base in the vertical plane result from either cephalad or caudal malposition of the alar base. These may present unilaterally or bilaterally. A cephalic malposition exposes the columella more ( Fig. 4 A), whereas a caudal malposition causes hooding of the alar base, with decreased show of columella. If the alar base is wide and cephalically malpositioned, narrowing the alar base results in medial and caudal translocation of the base. Otherwise, removal of an elliptical area of skin from the upper lip at the junction of the alar base and the lip is planned. The incision is made in the alar-facial crease and continued around the base to the nostril sill. The size of the resected skin is determined by preoperative facial analysis based on life-sized photographs. It is essential to completely release the soft tissue contained in the alar thickness so that the alar base can be advanced. Otherwise, this procedure may elevate the upper lip instead of transposing the alar base caudally. A caudally malpositioned alar base is not common and more difficult to correct ( Fig. 4 B). An incision is made in the vestibular lining just above the alar rim, and a strip of the lining is resected and repaired to reposition the alar base.
Horizontal alar base deformities are intricately interlaced with those in the vertical plane. Narrowing the wide alar base often pulls the alar rim caudally, reducing the columella-alar vertical discrepancy. For those who have retracted alae (ie, those with a cephalic malposition), this is beneficial to their nasal aesthetics. In those with caudal malposition, this medial movement of the ala during narrowing the alar base would be detrimental to the nasal harmony.
Vertical plane alar base deformities
Disharmonies of the alar base in the vertical plane result from either cephalad or caudal malposition of the alar base. These may present unilaterally or bilaterally. A cephalic malposition exposes the columella more ( Fig. 4 A), whereas a caudal malposition causes hooding of the alar base, with decreased show of columella. If the alar base is wide and cephalically malpositioned, narrowing the alar base results in medial and caudal translocation of the base. Otherwise, removal of an elliptical area of skin from the upper lip at the junction of the alar base and the lip is planned. The incision is made in the alar-facial crease and continued around the base to the nostril sill. The size of the resected skin is determined by preoperative facial analysis based on life-sized photographs. It is essential to completely release the soft tissue contained in the alar thickness so that the alar base can be advanced. Otherwise, this procedure may elevate the upper lip instead of transposing the alar base caudally. A caudally malpositioned alar base is not common and more difficult to correct ( Fig. 4 B). An incision is made in the vestibular lining just above the alar rim, and a strip of the lining is resected and repaired to reposition the alar base.






