19 Aesthetic Principles and Consultation
Minimally invasive aesthetic procedures have become the treatments of choice for rejuvenation of aging skin and facial enhancement.1 Since approval of botulinum toxin, dermal fillers, and lasers by the Food and Drug Administration (FDA) for cosmetic use, there has been a shift away from more traditional invasive surgical procedures that may radically alter appearance toward procedures that can enhance appearance in more natural and subtle ways. According to statistics from the American Society for Aesthetic Plastic Surgery, over 10 million aesthetic procedures are performed in the United States and more than 80% are minimally invasive.2 The most commonly performed procedures include onabotulinumtoxinA (Botox; formerly known as botulinum toxin type A) and dermal filler injections for treatment of wrinkles; lasers and intense pulsed light technologies for hair reduction, skin resurfacing, and photorejuvenation; and chemical peels and microdermabrasion for exfoliation.
These aesthetic procedures are associated with high patient and provider satisfaction because they are efficacious, have low risks of side effects, involve minimal patient discomfort with short recovery times, and can be safely performed in the office setting.3,4 As the popularity and demand for minimally invasive aesthetic procedures continues to grow, more health care providers are choosing to incorporate these types of treatments into their practice. This introduction to the aesthetic section of the book presents basic aesthetic principles for providers who wish to get started with aesthetic medicine. The succeeding chapters demonstrate the most commonly performed aesthetic procedures that can be readily incorporated into office practice.
Facial Aging
Facial aging is associated with a gradual thinning of the skin and loss of elasticity over time accompanied by the diminishment of dermal collagen, hyaluronic acid, and elastin. Ultraviolet (UV) radiation from sun exposure accelerates this process at a higher rate than does chronologic aging. This UV aging process is termed photoaging. To appreciate the contribution of photoaging to the appearance of aged skin, one needs only compare photoprotected skin, such as skin on the inside of the upper forearm or under the chin, to the appearance and texture of skin on face and back of the hands. Photoaged skin typically exhibits the following changes (Figure 19-1 for a computer-enhanced image demonstrating these signs)5:
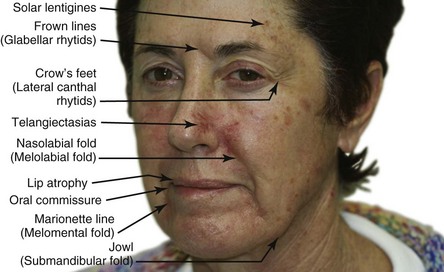
In a study by New York plastic surgeon Dr. D. Antell on aging in identical twins, extrinsic factors, such as prolonged sun exposure, resulted in advanced aging changes (Figure 19-2A) relative to the intrinsic aging seen in non–sun-exposed twins (Figure 19-2B).6 Habitual facial expressions also contribute to formation of visible lines and wrinkles, particularly in the upper one-third of the face, because repetitive muscle contractions etch in frown lines between eyebrows and crow’s feet radiating from the corner of the eyes. In addition to skin laxity, volume loss, and dynamic musculature, facial aging also results from biometric facial changes such as descent of malar fat pads, which contributes to deepened nasolabial folds, and resorption of maxillary and mandibular bone, which contributes to radial lip lines and mental crease formation.7,8

Skin Anatomy
The skin is divided into three layers: the epidermis, dermis, and hypodermis or subcutaneous layer (Figure 19-3). The epidermis is the top layer of the skin and is composed of four cell types: keratinocytes, melanocytes, Langerhans cells, and Merkel cells. The epidermis is further divided into the outermost nonliving layer, the stratum corneum, and the living cellular layers of the stratum granulosum, stratum spinosum, and stratum basale.
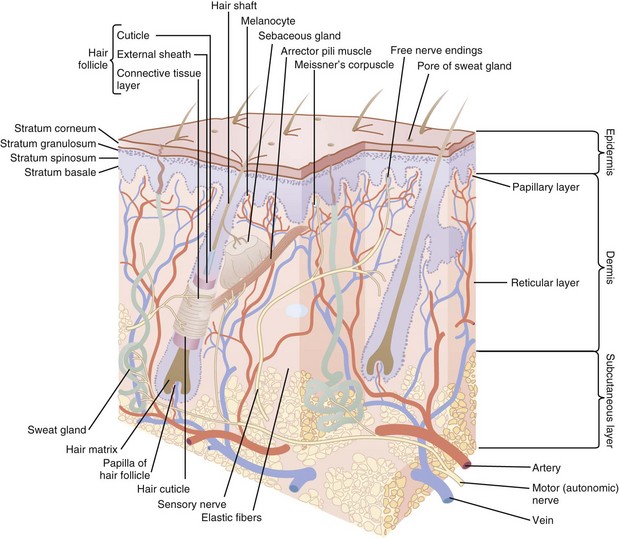
FIGURE 19-3 Skin anatomy.
(Modified from White CR, Bigby M, Sangueza OP. What is normal skin? In: Arndt KA, LeBoit PE, Robinson JK, Wintroub BU, eds., Cutaneous Medicine and Surgery. Philadelphia: Saunders; 1996:3–41.)
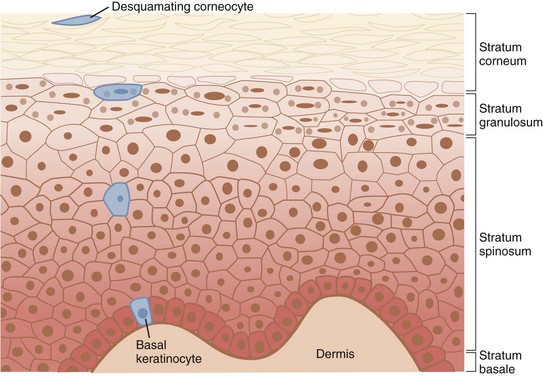
The stratum corneum is composed of corneocytes and lipids, which serves as a barrier against microbial pathogens and environmental irritants and also keeps the skin hydrated and protected from injury. Constant renewal is necessary for the epidermis to maintain its integrity and function effectively. In healthy young skin, it takes approximately 1 month for keratinocytes to migrate from the living basal layer of the epidermis to the stratum corneum surface and desquamate, during the process of epidermal renewal. Figure 19-4 shows the structure of the epidermis with the keratinocyte maturation highlighted. Photoaged skin demonstrates slower keratinocyte maturation and abnormal retention of cells in the epidermis. This results in a rough and thickened stratum corneum with impaired barrier function, reduced hydration capabilities, and increased pigmentation from retention of melanin-laden keratinocytes in the epidermis.
The distribution of melanin within the epidermis determines skin coloration. While the number of melanocytes is similar for both light and dark skin types, melanin is concentrated in small aggregated melanosomes in light skin and is more disbursed in darker skin.9
Aesthetic Consultation
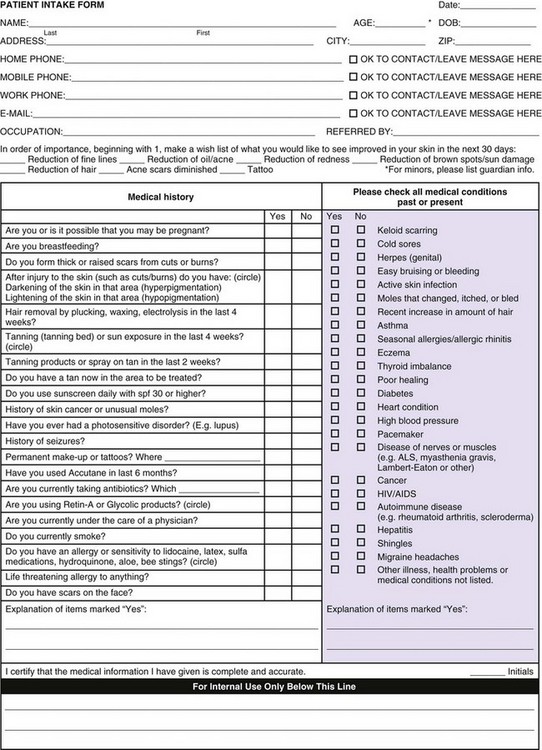
Aesthetic consultation is an important part of successfully performing aesthetic treatments. The patient’s medical history is reviewed, including past medical history, medications, allergies, and past cosmetic history (including results from previous treatments and side effects if any, surgeries, and satisfaction with outcomes). Figure 19-5 is an example of an aesthetic intake form that clinicians may use. Repeated dissatisfaction with past aesthetic treatments can be associated with unrealistic expectations or body dysmorphic disorder and is a contraindication to treatment.
The main areas of concern should be determined and prioritized by the patient at the time of consultation. It is recommended that the patient view these areas using a handheld mirror, so that the provider and patient may simultaneously examine the desired treatment areas. Asymmetries, such as uneven eyebrow height, are pointed out to the patient, noted in the chart, and photographed.10 Pigmented lesions in the treatment area are evaluated and lesions suspected of melanoma biopsied with results reviewed prior to proceeding with treatments.
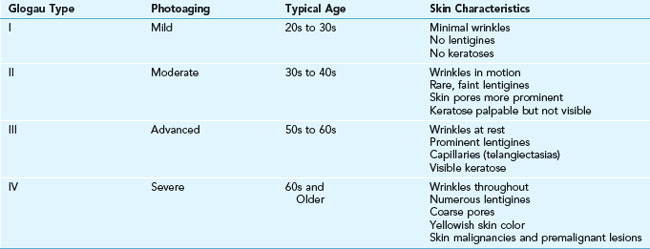
Glogau Classification of Photoaging
The Glogau classification system was developed to assess the severity of photoaging, especially with regard to wrinkles (see Table 19-1). It is used as a baseline measure at the time of aesthetic consultation and may be used as a gross guide to therapy. In general, Glogau types I, II, and III tend to show the most noticeable improvements with less aggressive minimally invasive aesthetic treatments such as botulinum toxin and dermal filler injections, nonablative lasers, superficial and fractional ablative lasers, and superficial skin resurfacing procedures such as light chemical peels and microdermabrasion. Glogau type IV patients often require deep ablative laser treatments and/or surgery for significant results.