Key points
• The anterior and posterior ethmoid foramen are the intraoperative anatomical landmarks to visualize for the level of a subcranial osteotomy. Violation of the frontal bone via an orbital osteotomy above these landmarks carries the risk of cerebrospinal fluid leakage due to exposure of the dura of the frontal lobe.
• The lateral canthus can be reliably resecured, but restoring the medial canthus can be problematic, and recreating the aesthetic position and contours of a natural medial canthus can be difficult if it becomes detached during the course of the procedure.
• The periorbital osteotomy must be posterior to the lacrimal crest and inferior to the turbinate to avoid injuring the nasofrontal duct.
• The infraorbital foramen marks the intraoperative landmark for the level of the maxillary–zygomatic osteotomy for repositioning the orbit.
• The orbital anatomy is best assessed through helical CT at approximately 0.5 mm slices.
• To translocate the ocular globe, the osteotomy must be carried out as posterior as technically possible; generally, the level is at the anterior two-thirds of the bony orbit to “carry” the globe, defined by Tessier as the “effective” orbit.
• In the patient who exhibits orbital dystopia in addition to facial asymmetry, the orbital surgery should be performed before corrective orthognathic surgery.
• The advent of computer-assisted surgical guides can improve the execution of the procedure, but, ultimately, the results are dependent on the surgeon’s ability to visualize the ideal in all three dimensions and the technical execution of a complex movement.
Introduction
Of all the components of our face, it is our eyes that define us. When the eyes and the orbits no longer have symmetry, the asymmetry involves the frontal region superiorly and inferiorly to the midface and the lower face as well. In addition to symmetry, the position of the orbits relative to each other and relative to the dominant central feature, the nose, often affects whether the face is perceived as normal or not. Equally, the position of the ocular globe relative to the skeletal framework of the bony orbit defines normality.
Of all the surgical procedures that require facial reconstruction, the hardest to master is the restoration of the human orbit because it involves (1) normalizing the position of the ocular globe within its skeletal orbital framework; (2) establishing orbital symmetry with its counterpart in all their planes (coronal, sagittal, and transverse); (3) positioning the orbits within normative facial proportions; and (4) finally, restoring the “normal anatomy” of the nose because it defines the mirror image line of symmetry. It is only after orbital symmetry and proportions are established that the remaining facial surgery (mid- and lower face) can be appropriately executed by using the orbit (horizontal axis) and the nose (vertical axis) as the reference axes.
Surgical anatomy of the orbit
The orbit is defined by seven bones: zygoma, maxilla, sphenoid, ethmoid, palatine, lacrimal, and frontal bones. Its overall shape approximates a “pyramid” with a rectangular base as the orbital rim and the apex as the optic foramen.
Orbital metrics
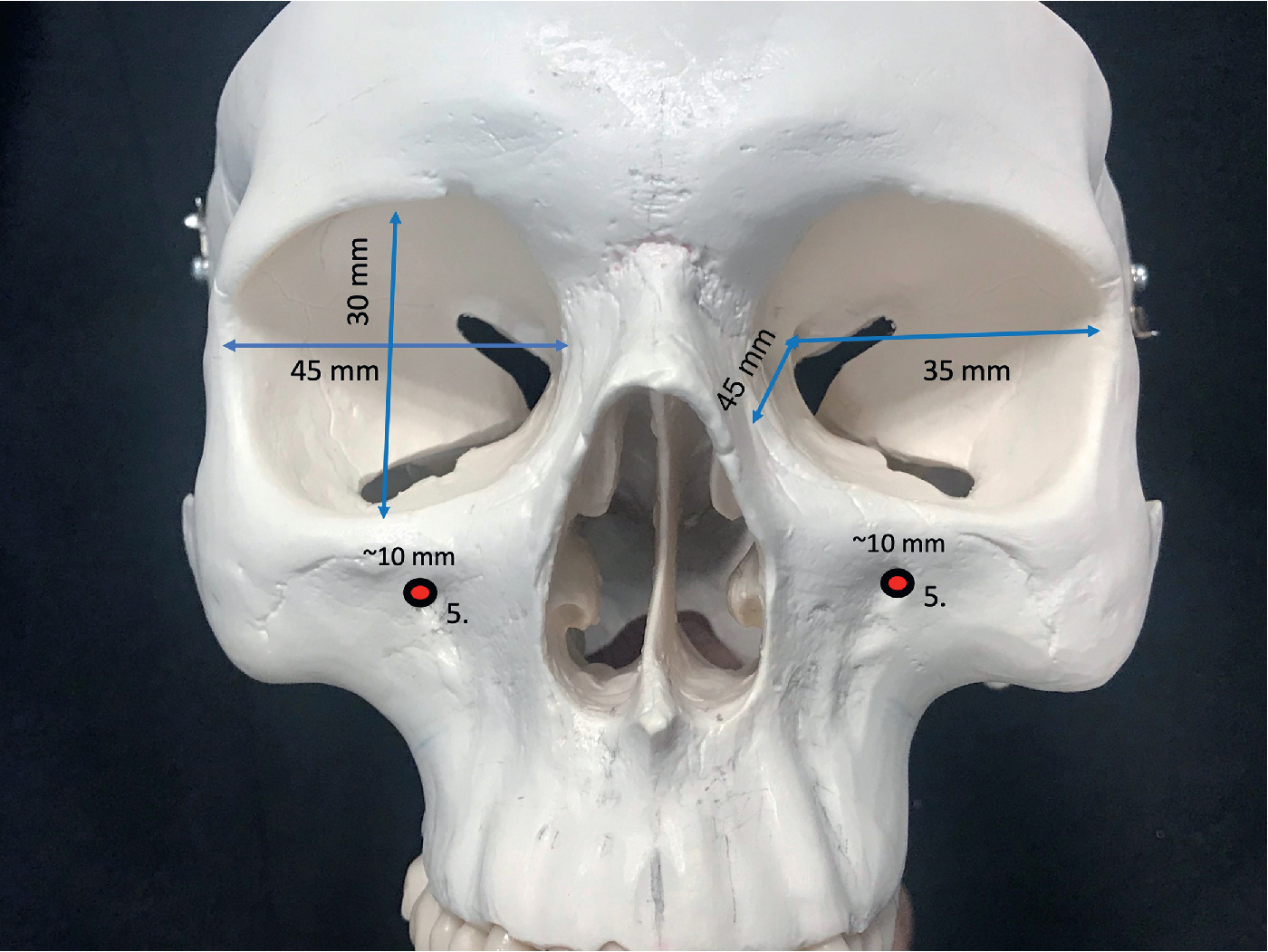
Although the orbit has a range of dimensions, it is important for the surgeon to have an understanding of approximate distances and angles that will be relevant for surgical planning and intraoperative guidance to critical landmarks ( Fig. 33.1 ). The orbital rim measures approximately 40 mm in length and 35 mm in height and has a lateral rotation in the transverse plane. From the medial orbital rim to the orbital apex, the depth of the pyramid is approximately 45 mm. From the lateral orbital rim to the orbital apex, the depth measures approximately 35 mm. The orbit expands at its widest circumference approximately 10 mm behind the orbital rim at the lacrimal recess. In the transverse plane, the medial orbital walls are parallel to the midsagittal plane, and the lateral orbital wall is approximately 45 degrees. Thus the left and right lateral orbital walls form a 90-degree angle. This lateral rotation places the lateral orbital rim approximately at the globe equator, exposing the eye. The medial orbital walls are separated by the paired medial ethmoid sinuses, and distance between the medial orbital walls is approximately 25 mm. The orbital volume is approximately 30 mL, and the volume of the globe that occupies it is approximately 7 mL.
Medial orbital wall
The medial orbital wall extends from the anterior lacrimal crest to the orbital apex. The anterior edge is demarcated by the lacrimal fossa, defined by the thick anterior and posterior lacrimal crest into which the medial canthal ligaments insert. Thereafter, the thin lamina papyracea separates the ethmoid sinus from the orbital contents. The medial orbital wall’s posterior edge is demarcated by the thick sphenoid bone that contains the optic canal. The area between the posterior lacrimal crest and the sphenoid, the lamina papyracea, is sectioned/fractured for the decompression procedure or for the medial wall osteotomy in translocation. The medial orbital wall’s upper edge is defined by the frontoethmoid suture that separates the intracranial cavities from the extracranial cavities. The anterior and posterior ethmoid foramen, through which the respective vessels course, are the intraoperative anatomic landmarks useful for the surgeon to visualize for the level of the osteotomy if the planned procedure is to remain subcranial ( Fig. 33.2 ). The vessels should be electrocauterized to prevent postoperative epistaxis and the foramen marked. Violation of the frontal bone via an orbital osteotomy above this suture carries the risk of cerebrospinal fluid leakage due to exposure of the dura of the frontal lobe.
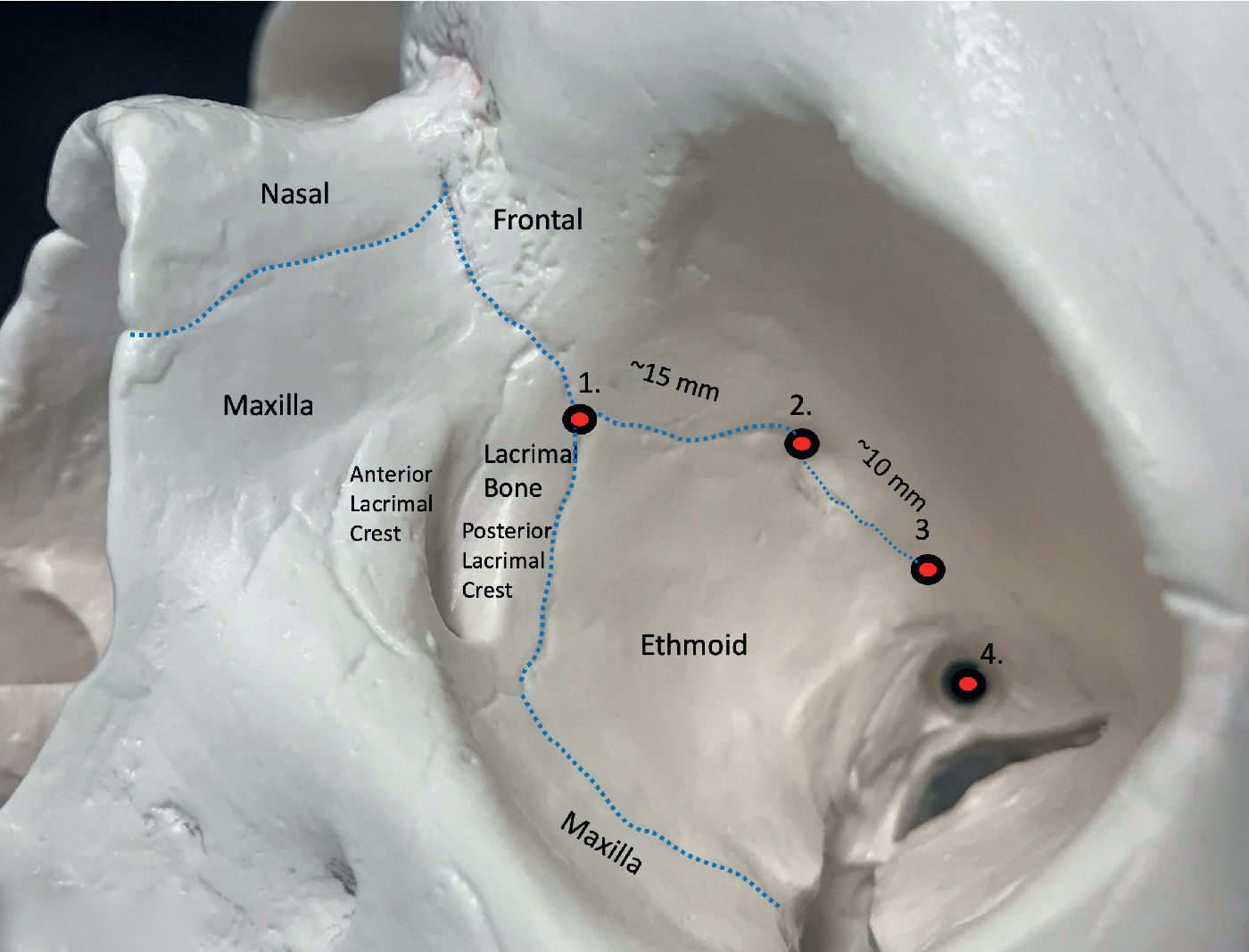
The medial canthus consists of a tendinous attachment of the orbicularis oculi muscle and a ligamentous attachment to the tarsus. The attachment is primarily at the anterior lacrimal crest, which is located on the frontal process of the maxilla. The posterior or minor contributor to the attachment is the posterior medial canthus, known as the pars lacrimal muscle or Horner muscle. This posterior limb also represents the attachment of the orbicularis oculi muscle to the posterior lacrimal crest. The lateral canthus can be reliably resecured, but restoring the medial canthus can be problematic, and recreating the aesthetic position and contours of a natural medial canthus can be difficult if it becomes detached during the course of the procedure. Once detached, canthal symmetry between the left and right medial canthus is difficult to achieve. Any discrepancy in the medial contours and a difference in position that exceeds 2 mm are noticeable because of their proximity to one another.
Located between the lacrimal bone and wedged between the anterior and posterior tendons is the nasolacrimal canal. Just above the canal is the lacrimal sac, which receives contributions from the lacrimal canaliculi to the nasolacrimal duct (see Fig. 33.2 ). The nasolacrimal duct courses within the inferomedial orbital wall from the lacrimal crest to its opening beneath the inferior nasal concha. The periorbital osteotomy must be posterior to the lacrimal crest and inferior to the turbinate to avoid injuring the nasofrontal duct. In some instances, placing a nasofrontal duct stent just before the osteotomy can be beneficial if there is potential risk to the duct.
Orbital floor
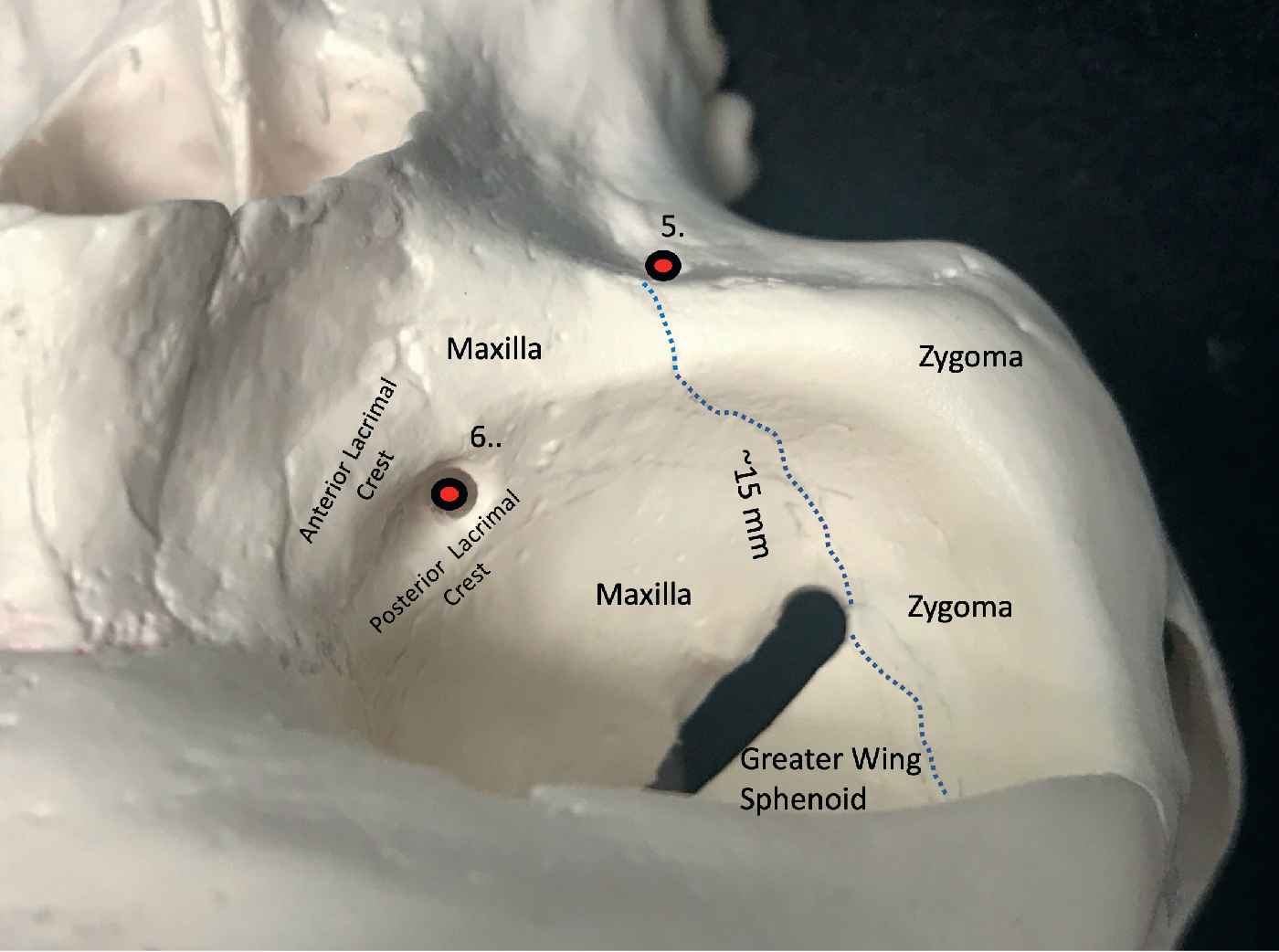
The orbital floor is composed of the orbital plate of the maxilla, the zygoma anterolaterally, and the palatine bone at its posterior-most limit. The orbital floor rises upward from anterior to posterior to merge with the medial orbital wall at the maxillary–ethmoid suture. This marks the position of the thick inferomedial bony strut that is left intact to support the globe and to prevent descent of the globe in cases of orbital decompression. From the inferior orbital rim, the floor initially dips inferiorly for approximately 15 mm, past the inferior orbital fissure. It then rises cephalically toward the superior orbital fissure. The floor rises steeply posterior to the globe equator to hold the globe forward. Understanding this rise in the elevation of the orbital floor is critical to correcting the relative position of the globe to the orbital rim. Without recreating the proper “rise” posterior to the globe, the correct position of the globe relative to its bony housing cannot be established. Approximately 10 to 15 mm posterior to the inferior orbital rim is the anterior edge of the inferior orbital fissure that separates the floor from the lateral wall and through which the maxillary division of the trigeminal nerve (V2) courses ( Fig. 33.3 ). The anterior edge is an intraoperative landmark for the surgeon to determine the depth of the orbital osteotomy when translocation is planned. V2 lies within the sulcus of the inferior orbital fissure, and as it courses anteriorly, it enters a bony canal and exits through the infraorbital foramen approximately 5 mm below the orbital rim. The infraorbital foramen marks the intraoperative landmark for the level of the maxillary–zygomatic osteotomy for repositioning the orbit.
Lateral orbital wall
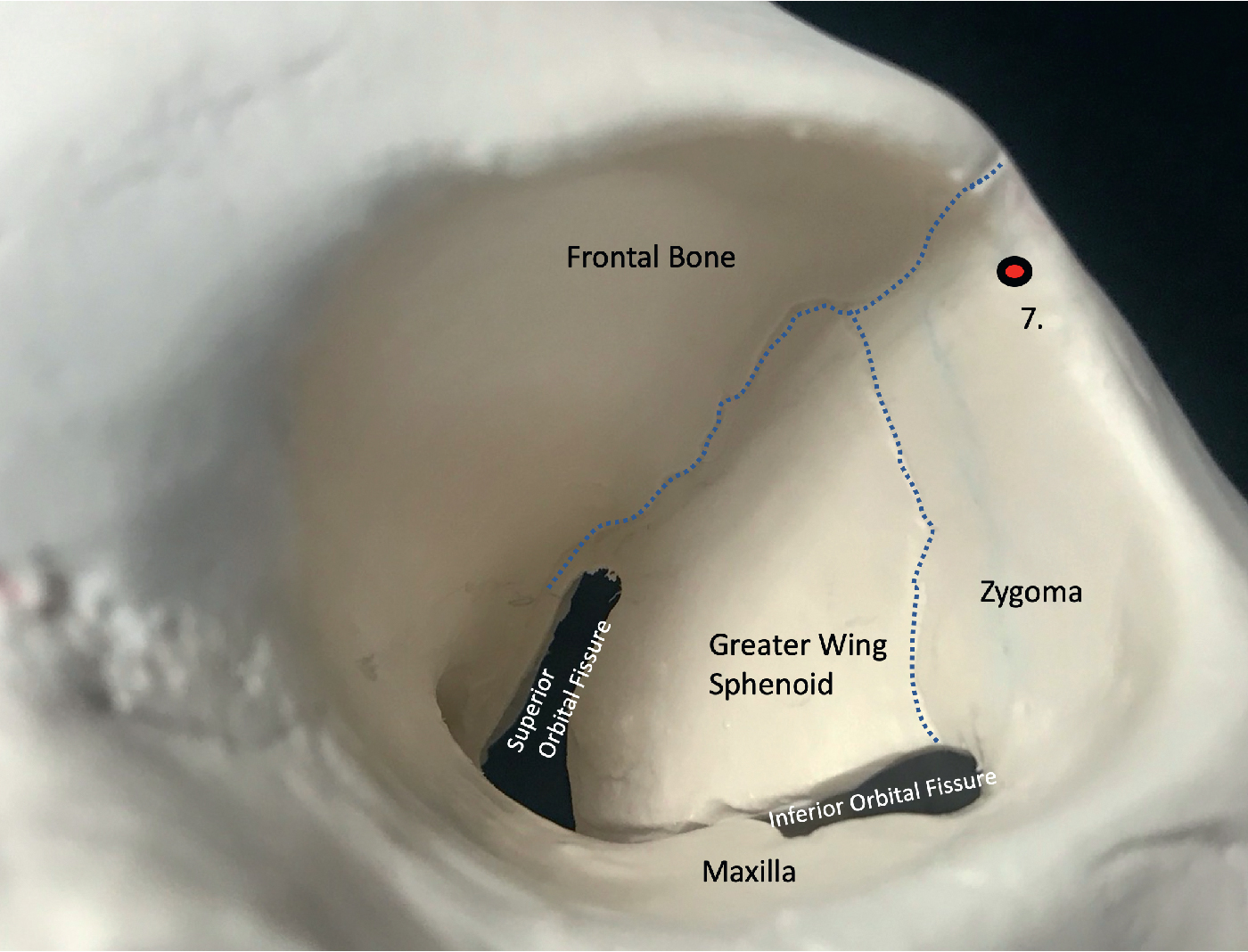
The lateral wall is formed by the zygoma anteriorly and by the greater wing of the sphenoid posteriorly. Unlike the thin medial orbital wall, the lateral orbital wall is substantially thicker. The lateral wall is separated by the orbital floor, the inferior orbital fissure, and the roof by the superior orbital fissure (posteriorly) and the frontosphenoid suture. The wing of the sphenoid separates the middle cranial fossa from the intraorbital and extracranial regions. The inferior orbital fissure is the intraoperative landmark that is used for the depth of the orbital osteotomy and, as the osteotomy is continued superiorly, becomes intraosseous within the sphenoid wing. The middle cranial fossa can be inadvertently breached through the sphenoid wing because it is shallow in many of the syndromic cases.
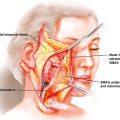
The Whitnall tubercle is located on the lateral orbital wall just inferior to the frontozygomatic suture and approximately 3 to 5 mm posterior to the lateral orbital rim ( Fig. 33.4 ). Its importance is that the lateral canthal tendon, the Lockwood ligament, and the check ligament of the lateral rectus attach at the tubercle. With orbital exposure, the lateral canthus is detached and will require resecuring to the Whitnall tubercle at its new position.
A number of vessels course through the lateral orbital wall will require cauterization. The zygomaticofacial and zygomaticotemporal neurovascular structures exit the orbit via their respective foramina on the lateral wall. Although encountered rarely, the surgeon should be aware of the one or more recurrent meningeal branches of the ophthalmic artery (internal carotid supply) that exit the orbit via the frontosphenoid suture to anastomose with the middle meningeal artery (external carotid supply).
Vocabulary of the orbits
The vocabulary of orbital surgery must be mastered by the surgeon. We begin by defining the relationship of the ocular globe to its skeletal framework. The terms exorbitism, exophthalmos, and proptosis are often used interchangeably to describe an eye that is abnormally protrusive beyond the confines of the orbital cavity. The term exophthalmos describes protrusion of the eye caused by an increase in orbital soft tissue contents but a normal bony orbit, as in Graves disease. When the volume of the orbital soft tissue is normal and the orbital cavity is of decreased capacity, the term exorbitism is often used, as in congenital cases of craniofaciosynostosis. The term enophthalmos is used when the volume of the orbital soft tissue is normal and the volume of the orbital cavity is increased, which is seen in traumatic conditions. Table 33.1 summarizes the dimensions of the “average” orbit.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


