The Clinical Problem ( Fig. 37.1 )
The hand is a major organ of the body. It is a sensory organ that has locomotor function and is used as a means of communication and assessing social status. The features of an aging face are in many ways similar to the features of an aging hand. Both show degenerative features in the skin as well as a reduction in the volume and consistency of tissue. Both are prone to the ravages of sun exposure. In the hand, skeletal joint changes in the form of arthritis can cause functional restriction, as well as deformity. Despite the hand being an important aesthetic unit in its own right, rejuvenation of the face, breasts, and trunk frequently takes priority for most patients.

Skin changes to the hand occur naturally over the passage of time but can be influenced by sun exposure, occupation, and genetics. In intrinsic aging, the skin may feel dry, develop fine wrinkles, and appear smooth and pale. Pigmented lesions usually arise from photo-aging of the skin. The epidermis thins, with flattening of the dermoepidermal junction, keratinocytes are less proliferative, and the skin can feel dry and rough. Dermal and epidermal thinning combined with less active or fewer melanocytes make the skin appear paler and shiny. The underlying vessels can be disrupted with minor trauma, presenting with ease of bruising due to capillary fragility. The skin on the dorsum of the aging hand is more prone to shear forces, and minor trauma can break the integrity of the skin in older adults. Surprisingly, though, such wounds invariably heal well.
In vasospastic disorders, botulinum toxin has been used to enhance the blood supply to the digits by blocking release of autonomic neuromuscular transmitters within the digital vessels , subsequently improving the appearance of the skin. Even in the absence of disease, there is small muscle atrophy and fat volume reduction naturally in the hand, both to the dorsal and palmar surfaces, appearing as guttering between the metacarpals and generalized wasting with skin wrinkling and thinning ( Fig. 37.2 ). Arthritic changes or nerve entrapment resulting in reduced muscle activity can also contribute to this appearance.

Other lesions such as actinic keratosis and basal papillomas are commonly seen in photo-aging, as are variants of malignancy, from Bowen disease to full squamous cell carcinomas.
Surgical Preparation and Technique
Management of the Aging Hand
The management of the aging hand can be considered as nonsurgical (e.g., camouflage, cosmoceuticals, fillers, Botox, skin resurfacing) and surgical (e.g., lipofilling, removal visible veins and excisional).
Nonsurgical Management
Camouflage acts purely as a cover film over the epidermis temporarily but visibly improves the appearance. Cosmoceuticals are purported to reduce fine wrinkles. These are creams or lotions with additives such as products based on vitamins A, C, D, and/or E. These agents have been theorized and shown in vitro to influence the proliferation of keratinocytes, but the clinical effectiveness of these products is somewhat subjective, is often influenced by market forces, and lack evidence base. Retinoids (vitamin A) have been used for the treatment of psoriasis, acne, and actinic keratosis.
Dorsal hand skin can be lasered or subjected to cryotherapy for age-related spots. Thickened scars have also been treated with these modalities, although scars are usually treated with topical silicone rather than with triamcinolone steroid injections because fat atrophy, pigment loss, skin thinning, and telangiectasia may occur.
Volume loss is often the primary presenting complaint. In this situation, a nonpermanent filler is the safest initial approach because any change of heart is easily redeemable simply by waiting and allowing the agent to be broken down. Fillers can injected into the skin or subcutaneous tissue, thereby altering contour to achieve an aesthetically desirable appearance. However, these may be more visible and lumpy.
Hyaluronic acid is the gold standard because it is naturally occurring and potentially reversible with hyalase. Its effects can last for more than 1 year.
Sclerotherapy is the most widely used medical procedure for the ablation of varicose veins and spider veins or capillary hemangiomas causing endothelial damage and ultimately fibrosis. Usually, the sclerosant is shaken to create a foam. The most common detergent sclerosants are polidocanol and tetradecyl sulfate. They are called detergent sclerosants because they are active as micelles and have a low incidence of allergic reactions and staining caused by hemosiderin deposition.
Skin-resurfacing topical chemical agents can provide a controlled resurfacing of the skin but the deeper the peel, the greater the risk of visible scarring and depigmentation. A deeper peel may be produced by a prolonged single application of a more concentrated agent or, more superficially, by the use of milder fruit acid peels. The standard peeling agent is trichloroacetic acid (TCA), which provides a variable depth injury by varying its topical concentration and contact time on the skin. Other peeling agents may be toxic, such as phenol and salicylic acid.
Surgical Management
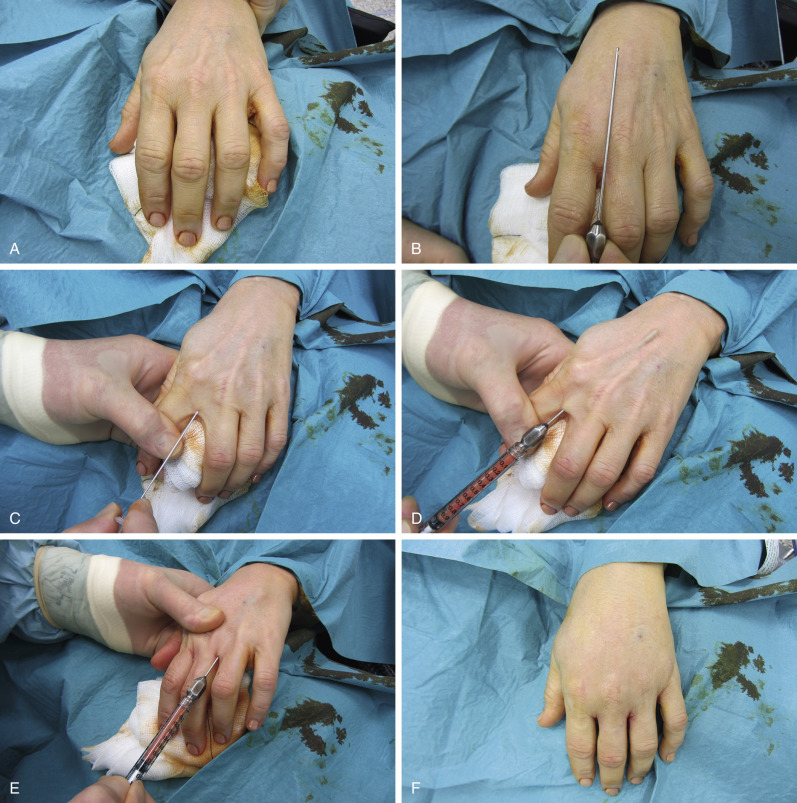
Fat grafting uses autologous tissue and is potentially a permanent filler that softens contours. Aging skin seems to improve in quality after fat grafting. It is an extremely good filler to correct neuropathic wasting, such as the thenar eminence in long-standing carpal tunnel syndrome, where there is irreversible atrophy of the abductor pollicis brevis. Similarly, it can be used for the hypothenar eminence and for intermetacarpal guttering and the first web space resulting from wasting to the small muscles secondary to ulnar nerve palsy. Small volumes of fat (up to 20 mL) are harvested using the tumescent Coleman technique. I prefer the harvested fat to separate gravitationally in a 10-mL aspiration syringe by standing rather than separation by centrifuge and then titrate or filter away the unwanted oily and crystalloid layers. A 1-mL syringe and blunt cannula are used for injection of fat via the dorsal web spaces, taking care to avoid damaging the dorsal veins. The fat is layered to lie adjacent to the veins within the dorsal gutters to mask the prominence of the veins. The injection sites should be selected with obvious care to avoid damage to nerves, vessels, and tendons ( Fig. 37.3 ). Fat is harvested from a region that does not vary significantly in volume with weight variation; the choice is negotiated with the patient. Patients are warned that the process may need to be repeated to allow for variable fat loss. The outcome is usually apparent at 6 months.