Support of the lower eyelid with canthal suspension is a useful tool in the prevention of complications of lower blepharoplasty, particularly for eyelids with increased lower lid laxity, relatively prominent globes, and negative vector configuration of the eyelid-cheek junction. Management options include canthopexy, orbicularis sling, and modified canthoplasty. The most conservative option is canthopexy, which supports the lower eyelid over the short or long term. The orbicularis sling technique avoids surgery around the lateral canthus, but may not be suitable for some cases. Canthoplasty is generally reserved for more marked laxity, which is less common in patients seeking aesthetic blepharoplasty.
Key points
- •
Aesthetic canthal suspension is defined as a lateral elevation of the lower eyelid, which may be completed as an independent procedure or more commonly in conjunction with aesthetic lower blepharoplasty.
- •
Indications for suspension of the lower eyelid include facial aging, laxity of the lower eyelid, and prevention of lower eyelid malposition.
- •
Preoperative evaluation of the lower eyelid and its position with respect to the globe and the cheek is key to optimal surgical management.
- •
Anatomy of the lower eyelid and lateral canthus is both intricate and complex; thorough understanding of anatomy is required to avoid complications in aesthetic canthal suspension.
- •
Canthopexy is defined as a procedure to elevate and support the lower eyelid to the lateral orbital rim with a plication suture without modification of the canthal tendon.
- •
Canthoplasty is defined as a procedure that modifies, tightens, and can shorten the lower eyelid, and may involve surgery on the lateral canthal tendon, tarsus, and orbicularis oculi.
- •
Risk of major complications of lower eyelid surgery including lower eyelid retraction and ectropion, may be reduced with aesthetic canthal suspension.
Overview
Laxity of the lower eyelid is a common characteristic of facial aging, and correction of lower eyelid laxity in conjunction with aesthetic blepharoplasty is key to both an optimal cosmetic outcome and avoidance of surgical complications. Laxity of the lower eyelid is evaluated preoperatively with the snap-back test. When lower eyelid blepharoplasty is completed with either a transcutaneous or transconjunctival technique, consideration must be given to the need for lower eyelid support to avoid potential complications including lower eyelid retraction and ectropion. With particular relevance to transcutaneous lower blepharoplasty, excision of lower eyelid skin without consideration of canthal suspension results in an increased risk of lower eyelid retraction or malposition. Aesthetic canthal suspension may involve a single support suture to support the lower eyelid from the lateral orbital rim (canthopexy) or support of the lateral canthal tendon (canthoplasty), or tightening of the orbicularis oculi (orbicularis sling). Care is required in support and alteration of the lateral canthus, as small differences can be apparent with asymmetry or functional discomfort.
Oculoplastic surgeons have a good anatomic knowledge of this area, as reconstructive surgery on the lateral canthus is a common procedure. By contrast, other surgical specialties often find this area challenging because the anatomy is intricate and less familiar. As a consequence, the orbicularis sling technique, which avoids intricate surgery on the lateral canthus while providing lateral canthal suspension, is a technique preferred by some surgeons. This article aims to provide a practical application for surgeons in performing aesthetic canthal suspension.
Overview
Laxity of the lower eyelid is a common characteristic of facial aging, and correction of lower eyelid laxity in conjunction with aesthetic blepharoplasty is key to both an optimal cosmetic outcome and avoidance of surgical complications. Laxity of the lower eyelid is evaluated preoperatively with the snap-back test. When lower eyelid blepharoplasty is completed with either a transcutaneous or transconjunctival technique, consideration must be given to the need for lower eyelid support to avoid potential complications including lower eyelid retraction and ectropion. With particular relevance to transcutaneous lower blepharoplasty, excision of lower eyelid skin without consideration of canthal suspension results in an increased risk of lower eyelid retraction or malposition. Aesthetic canthal suspension may involve a single support suture to support the lower eyelid from the lateral orbital rim (canthopexy) or support of the lateral canthal tendon (canthoplasty), or tightening of the orbicularis oculi (orbicularis sling). Care is required in support and alteration of the lateral canthus, as small differences can be apparent with asymmetry or functional discomfort.
Oculoplastic surgeons have a good anatomic knowledge of this area, as reconstructive surgery on the lateral canthus is a common procedure. By contrast, other surgical specialties often find this area challenging because the anatomy is intricate and less familiar. As a consequence, the orbicularis sling technique, which avoids intricate surgery on the lateral canthus while providing lateral canthal suspension, is a technique preferred by some surgeons. This article aims to provide a practical application for surgeons in performing aesthetic canthal suspension.
Anatomy
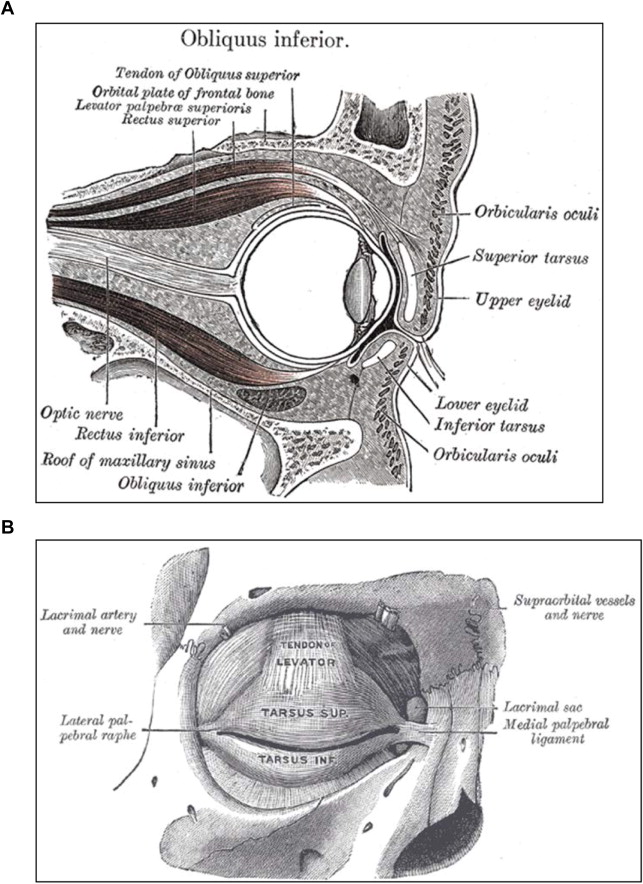
The lower eyelid is a mobile structure that protects the eye from injury and enables the even distribution of the tears on blinking. The eyelid consists of 3 principal layers ( Fig. 1 ):
- 1.
Anterior lamella (skin, subcutaneous tissue, orbicularis oculi muscle)
- 2.
Middle lamella (orbital septum)
- 3.
Posterior lamellar (tarsal plates, striated and smooth muscle, and conjunctiva)
Anterior Lamella
The eyelid skin is the thinnest in the body. Beneath the skin is loose subcutaneous tissue rich in elastic fibers and with minimal fat. The orbicularis oculi is a sphincteric muscle globe composed of elliptical fibers that surround the globe. It is divided into 2 principal segments:
- 1.
The palpebral part, which lies over the eyelids proper and is further subdivided into pretarsal and preseptal portions named after the anatomic eyelid structures beneath
- 2.
An orbital part whose fibers run concentrically over the orbital rim
The orbicularis oculi is a protractor of the eyelids whose function is to close the eyelids. The muscle is innervated from its undersurface by the temporal (upper eyelids) and zygomatic (lower eyelids) branches of the facial nerve.
Middle Lamella
The orbital septum is a fibrous structure beneath the orbicularis muscle, which divides the anterior lamella from the orbital cavity. It is a continuation of the periosteum at the orbital rim. Vertically the septum fuses with the lower eyelid retractors 5 mm below the tarsus, continuing as one layer until inserting on the inferior edge of the tarsus. Horizontally the septum lies posterior to the medial palpebral ligament (canthal tendon) and anterior to the lateral palpebral ligament. The orbital septum provides an important functional barrier in the eyelid that protects the spread of infection from superficial skin tissues to the orbital cavity.
Posterior Lamella
The tarsal plates form a dense fibrous tissue that gives the eyelids a defined shape and structure. The tarsus in the lower lid measures approximately 3 to 4 mm in height (compared with 10 mm in the upper eyelid) and 20 mm in length, and is attached medially via the medial palpebral ligament to the lacrimal crest and laterally to the Whitnall ligament.
Finally, the lower eyelid retractors form a fibromuscular structure composed of the capsulopalpebral fascia and inferior tarsal muscle. The retractors originate and are an extension of the inferior rectus muscle, and provide 3 to 5 mm of movement to the lower eyelid.
Lateral Canthus
The lateral canthus anatomically is where the upper and lower lids meet laterally. The point where the lids meet is called the commissure. The lateral canthal tendon, which bolsters the eyelids to the orbital rim, is formed by the pretarsal and preseptal portions of the orbicularis, which taper to form the superior and inferior limb of the lateral canthal tendon, which inserts onto the Whitnall tubercle 2 mm posterior to the lateral orbital rim. In most people the height of the lateral canthus is several millimeters above the medial canthus (see Fig. 1 ).
Blood Supply of the Lower Eyelids
- •
The eyelids have a profuse blood supply from the lateral and medial palpebral arteries that form a marginal and peripheral arterial arch in the upper and lower eyelids. The lateral palpebral arteries are derived from the lacrimal artery and the medical palpebral arteries from the ophthalmic artery. The venous drainage is to the superior orbital vein and the facial vein.
- •
The lymphatic drainage of the medial two-thirds of the lower eyelid is to the submandibular lymph nodes, and from the lateral one-third to the superficial parotid lymph nodes.
Related posts:
 An Algorithmic Approach to Multimodality Midfacial Rejuvenation Using a New Classification System for Midfacial Aging
An Algorithmic Approach to Multimodality Midfacial Rejuvenation Using a New Classification System for Midfacial Aging
 Dark Circles
Transconjunctival Lower Lid Blepharoplasty with and Without Fat Repositioning
The Transeyelid Midface Lift
Dark Circles
Transconjunctival Lower Lid Blepharoplasty with and Without Fat Repositioning
The Transeyelid Midface Lift
 Transtemporal Midface Lifting to Blend the Lower Eyelid-Cheek Junction
Autologous Fat Grafting for Midface Rejuvenation
Transtemporal Midface Lifting to Blend the Lower Eyelid-Cheek Junction
Autologous Fat Grafting for Midface Rejuvenation
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


