Breast augmentation has consistently been the most common cosmetic surgical procedure performed in the United States since 2006. Capsular contracture, the most common reason for implant removal and/or revision, can cause breast pain and discomfort and affect the breast. Revision surgery is associated with decreased patient satisfaction rates and capsular contracture recurrence. Why some capsules form and some progress to contracture is still subject to hypothesis. It has been theorized that capsular contracture results from an imbalance between suppressors and potentiators, favoring potentiators where an imbalance biased towards potentiators leads to capsular contracture.
Key points
- •
Current hypotheses suggest capsular contracture results from a multifaceted process with infection and biofilm formation strongly implicated.
- •
Capsulectomy, implant exchange, and pocket switch with acellular dermal matrix maybe an important adjunct in treatment algorithms for Baker grade III/IV capsular contracture.
- •
Prevention strategies are being elucidated but clinical applications are currently limited.
Introduction
Breast augmentation has consistently been the most common cosmetic surgical procedure performed in the United States since 2006, with nearly 300,000 breast implant procedures conducted in 2019. Complications of breast implantation surgery include hematoma, seroma, infection, altered nipple sensation, asymmetry, scarring, rupture, and capsular contracture. Capsular contracture, the most common reason for implant removal and/or revision, , can cause breast pain and discomfort and affect the breast aesthetic, where contracture of the implant capsule causes a spherical conformity. The overall incidence of capsular contracture in patients with breast implant revision surgery in Australia was 39.1% to 41.6%. Revision surgery is associated with decreased patient satisfaction rates and capsular contracture recurrence. Why some capsules form and some progress to contracture is still subject to hypothesis. Adams theorized capsular contracture results form an imbalance between suppressors and potentiators, favoring potentiators.
Capsular contracture
Insertion of a breast implants induces a foreign body type reaction (FBR). FBR follows a 6-stage process of blood-biomaterial interaction, provisional matrix formation, acute inflammation, chronic inflammation, foreign body giant cell formation, and fibrous capsule formation. The peri-implant capsule consists of 3 layers: an inner layer, an intermediate layer with smaller fibrils and rich vascular network, and an outer collagen-dense layer. The underlying pathohistological mechanism potentiating capsular contracture remains to be elucidated despite numerous studies. Early histologic studies have characterized the inner capsule layer as a synovial metaplasialike layer with vimentin (mesenchymal) and CD 68 (macrophage) positivity. Loss of integrity of the inner layer has been correlated with increasing baker grade capsules.
Capsular contracture is graded by the Baker classification. Typically, patients with Grade III or IV will require operative intervention. Capsular contracture etiopathogenesis is likely to be a multifactorial process. Current proposed theories range from an inflammatory process possibly secondary to subclinical infection, an immune-mediated humeral response, myofibroblast activation, talc-induced fibrosis, dust, or silicone gel bleed. Surgical factors: pocket position and incision choice have been associated with capsular contracture.
Montemurro and colleagues, have identified capsular contracture affecting 3 successive generations of a family implicating a possible genetic predisposition.
Biofilms
A biofilm is an aggregate of microorganisms in which cells that are frequently embedded within a self-produced matrix of extracellular polymeric substance (EPS) adhere to each other and/or to a surface. Further understanding of biofilm formation has revealed a dynamic complex developmental process that evolves and adapts to environmental changes and challenges via a coordinated regulatory network.
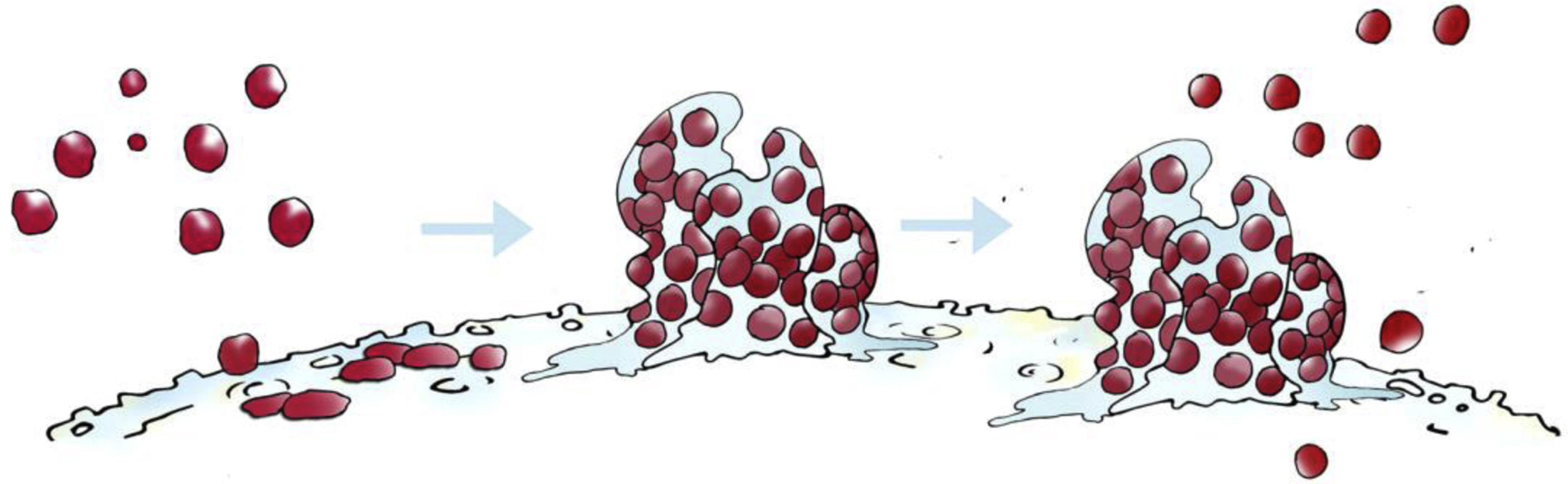
Formation of biofilm
Attachment
Bacteria exist in 2 states. They are either free-floating (planktonic) or attached (biofilm). Formation of biofilm begins with planktonic bacteria introduced to a surface. The ability of bacteria to associate with a surface is dependent on hydrodynamic forces, , environmental features: pH, temperature, and bacterial characteristics, for example, motility. Adherence is mediated by extracellular adhesion ligands, for example, pili and secreted products. The achievement of adherence marks the transition from a reversible, where bacteria may slough off or be propelled by nutrient factors to maintain a planktonic phase, to an irreversible phase. Pili, curli fibers, surface antigens, for example, antigen 43, and surface proteins have been demonstrated to be involved with adherence to abiotic surfaces in pseudomonas , and enterococci families.
Maturation
Attachment triggers the upregulation of genes imparting sessility and the formation of the extracellular matrix. , Extracellular matrix is composed of polysaccharides, proteins, nucleic acids, lipids and adhesive fibers. It functions to store nutrients and water and form a 3-dimensional scaffold to protect bacteria. This results in the formation of genetically discrete microcolonies that attached to each other and the surface. Upregulation of molecules along with extracellular DNA (eDNA) have been experimentally demonstrated to stabilize the extracellular matrix, , infer drug resistance, and evasion of host immune defences. Biofilms have multiple genetically distinct colonies, each self regulates its immediate extracellular matrix to regulate pH and nutrients in a homeostatic fashion to satisfy nutrient demand, regulate pH, and thus metabolic activity and so forth. Colonies with cells with variable metabolic activity, and heterogeneity of species and subspecies vastly complicate treatment avenues.
Dispersion
Dispersion is the point in development in which bacteria may leave the biofilm. This can be passive and secondary to shear forces or active. A shift to resume a planktonic state maybe due to environmental stresses such as nutrient availability, oxygen source, or toxic metabolite buildup ( Fig. 1 ).
Biofilm has been recognized since the late 1970s and may be implicated in up to 80% of infections Biofilm-associated infections are difficult to treat, and their persistence can lead to chronic and recalcitrant infections. The biofilm acting in concert uses a varied and dynamic arsenal to evade the host environment. Features of the extracellular matrix along with the conjugation of genetic material permits drug resistance. Persister cells, within the biofilm remain in a state of quiescence while maintaining tolerance to antimicrobial challenge and are thought to be key in the reestablishment of biofilms after antibiotic therapy
Capsular contracture
Animal models first demonstrated a possible association between bacterial contamination of implants and capsular contracture in the 1980s. Further studies have since supported this association with a causal relationship elegantly demonstrated by Tamboto and colleagues. Human clinical studies have also documented strong correlations between the presence of biofilm and capsular contracture. , Coagulase-negative staphylococci were the principal organism, especially those of the Staphylococcus epidermidis group. Pajkos and colleagues also noted the presence of extensive inflammation in a proportion of the contracted capsule of breast implants with positive identification of biofilm.
Inflammatory response
The host immune system is composed of an innate (nonspecific) and adaptive (specific) response. Briefly, tissue trauma leads to activation of a clotting cascade and stimulation of pattern recognition receptors (PRRs) on host cells either by pathogen-associated molecular patterns (PAMPs) or damage-associated molecular patterns (DAMPS). This results in recruitment of phagocytic cells of the innate lineage and a proinflammatory cytokine profile (interferonγ and tumor necrosis factor [TNF]α) with the aim of clearing wound contaminates: bacteria and host cellular debris. Stimulated macrophages along with dendritic cells at the trauma interface are able to recruit the adaptive immune system via T-cell activation. T-cell activation is able to subsequently induce B-cell involvement and antibody production.
Biofilms are associated with an ongoing inflammatory response mediated by proinflammatory cytokines. Prolonged recruitment and stimulation of proinflammatory cells, for example, neutrophils, macrophages, and lymphocytes, may result in ongoing host tissue destruction and further release of inflammatory mediators. Furthermore, biofilms have been shown to use components of the immune response to enhance biofilm formation.
TGF-β has complicated and multifaceted effects on the immune system and has been implicated in chronic inflammation and has been described as a “master switch” in fibrosis. TGF-β stimulation results in myofibroblast differentiation, activation, and proliferation and in animal studies exogenous TGF-β or overexpression results in tissue fibrosis. ,
Mazhar and colleagues 2014 demonstrated a correlation among biofilm, TGF-β expression, and tracheal stenosis. Tracheal stent–associated biofilm was associated with increased expression of TGF-β and tracheal stenosis.
Biofilm may induce a chronic inflammatory state with upregulation of proinflammatory cytokines resulting myofibroblast activation and capsular contracture.
Breast implant associated–anaplastic large cell lymphoma
Breast implant–associated anaplastic large cell lymphoma (BIA-ALCL) was first reported by Keech and colleagues in 1997. Currently, BIA-ALCL is an entity associated exclusively with textured implants.
In vitro studies demonstrated increased rates of biofilm formation in textured implants compared with smooth implants. High and intermediate surface area implants have been shown to have a 10-fold increased incidence of BIA-ALCL compared with low surface area implants. Hu and colleagues demonstrated a linear relationship between bacterial load and number of activated lymphocytes, especially CD4+ lymphocytes and a gram-negative shift in the BIA-ALCL microbiome.
Several hypotheses have emerged in a bid to explain the association of bacteria BIA-ALCL. The lipopolysaccharide coat of gram-negative bacteria has been implicated in autoimmune diseases and may act as a malignant trigger. A Bacterial superantigen may initiate a profound cytokine release and exaggerated T-cell differentiation.
Gene expression profiling of tumorigenic lymphoid cells have suggested a T-helper 17 (Th-17) or innate lymphoid cell type 3 (ILC 3) cellular phenotype for systemic ALCL. , The presence of Th-17–associated cytokines and transcription factors in BIA-ALCL tissue for example, IL-17, ROR-y, and interleukin (IL)-26 further supports the possible role of Th-17 cells. Interestingly TGF-β has been isolated from BIA-ALCL cell lines.
Treatment
Classically the gold standard treatment of capsular contracture was total capsulectomy, pocket switch and implant replacement. The use of acellular dermal matrix (ADM) has been a useful adjunct to revision implant-based breast surgery and may prove an invaluable addition to the treatment algorithm.
Acellular Dermal Matric and Capsular Contracture
ADM was first introduced by Breuing and Warren in 2005 to increase outcomes following alloplastic breast reconstruction. ADM may function as a barrier between the implant and host defense system limiting inflammation and scarring. In vitro studies by Orenstein and colleagues demonstrated an inhibitory effect of AlloDerm on IL-1, IL-6, IL-8, and vacular endothelial growth factor (VEGF) production when placed in contact with peripheral blood mononuclear cells. Animal in vivo studies have demonstrated a reduced myofibroblast cell count and reduced capsule thickness. Although Human studies have demonstrated decreased fibrosis, fibroblast cellularity, and foreign body giant cell inflammatory reactions. Maxwell and Gabriel published a series of 186 patients undergoing revisional aesthetic breast surgery and demonstrated a capsular contracture recurrence rate of 1.6%. Salzberg and colleagues similarly demonstrated a decreased in capsular contracture rate in dual plane breast reconstruction with the use of ADM in a large cohort of more than 1500 patients over a 13-year period.
Prevention
A role for bacterial contamination in the pathogenesis of capsular contracture has resulted in the publication of techniques focused on maintenance of asepsis. Interventions have ranged from occlusive nipple shields, antimicrobial pocket irrigation fluids, , Intravenous antibiotics, and surgical technique including choice of incision and choice of pocket. , A 14-point plan was developed and evaluated in more than 42,000 implants. Adams and colleagues demonstrated an overall capsular contracture rate of 2.2% with implementation of the 14-point plan.
Advances in prevention of biofilm
Methicillin-resistant Staphylococcus aureus (MRSA)-associated biofilm formation identified a key role for host proteins. Urinary catheterization leads to bladder inflammation, fibrinogen secretion, and deposition on the catheter and bladder uroepithelium. MRSA infection was noted to colocalize specifically to areas of fibrinogen deposition. Furthermore, MRSA exacerbated the inflammatory response resulting in further fibrinogen deposition. Fibrinogen binding motifs, Clumping factor A and B, were identified. Inhibition or blocking of binding motifs may prevent biofilm formation.
This has been demonstrated by Flores-Mireles and colleagues. Enterococcus faecalis has a fibrinogen binding motif, EbpA. This motif facilitates binding to fibrinogen on urinary catheters and biofilm formation in the similar fashion as MRSA. Formation of biofilm and infection was prevented in mice vaccinated with EbpA compared with unvaccinated controls. Circulating anti-EbpA antibodies block binding of E faecalis to fibrinogen and formation of biofilm and infection.
Surface modification
Silicone is hydrophobic in nature; pocket irrigation solutions such as betadine and antibiotics are hydrophilic. Gas plasma sterilization, for example, with oxygen results in −OH group binding to silicone. Potentially this would facilitate a high affinity for polar molecules (povidone iodine and antibiotics) and thus prolong antimicrobial activity. Barnea and colleagues demonstrated increased antimicrobial activity of povidone-iodine and cefazolin on plasma-treated textured implants compared with untreated controls.
Steroids
Steroids have well-proven anti-inflammatory activity and are known to inhibit inflammatory cytokines. Glucocorticoids also downregulate adhesion molecules and chemoattractants ; this may reduce the invasion of macrophages and thus reduce TGF-β production. A pilot rat study by Jeon and colleagues demonstrated triamcinolone-coated textured implants reduced TGF-β expression, the number of fibroblasts and myofibroblasts, capsule thickness, and collagen density.
Transforming growth factor-β inhibition
Tranilast, a drug used in the treatment of asthma, is a known TGF-β intracellular signaling pathway inhibitor. Park and colleagues demonstrated a reduced capsule thickness and collagen density in textured implant coated with tranilast compared with uncoated controls in a rodent model.
Leukotriene antagonists
Leukotriene antagonist, montelukast, and zafirlukast inhibit cysteinyl leukotrienes (CysLTs). CysLTs are implicated in the migration of fibroblasts and promote their differentiation to myofibroblasts. Early in vivo rodent models have demonstrated a reduction of fibroblasts and reduced capsule formation ,
Summary
Valuable ongoing collaborative clinical and laboratory research will continue to advance our understanding of the complex pathogenesis of capsular contracture and potentially lead to the discovery of effective prevention strategies and the panacea of capsular contracture.
Disclosure
A.K. Deva is a consultant to Allergan, Mentor (J&J), and KCI. He has previously coordinated industry-sponsored research for these companies relating to both biofilms and breast prostheses.
References
Related posts:
 Breast Implant–Associated Anaplastic Large Cell Lymphoma
Breast Implant–Associated Anaplastic Large Cell Lymphoma
 Fundamentals of High-Resolution Ultrasound in Breast Implant Screening for Plastic Surgeons
Fundamentals of High-Resolution Ultrasound in Breast Implant Screening for Plastic Surgeons
 Moving Toward Opioid-Free Breast Surgery
Moving Toward Opioid-Free Breast Surgery
 An Algorithm for the Management of Explantation Surgery
An Algorithm for the Management of Explantation Surgery
 Mastopexy with Autoaugmentation and Fat Transfer
Mastopexy with Autoaugmentation and Fat Transfer
 Augmentation Mastopexy:
Augmentation Mastopexy:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


