Patients have been requesting implant removal in revisional breast surgery and options for breast improvement without the use of breast implants in primary breast surgery. This article focuses on perioperative decision making and surgical technique in performing a mastopexy with autoaugmentation and fat grafting. The use of a lower island of breast parenchyma relocated to the upper pole through a central pedicle in primary surgery and a superior pedicle in postexplantation cases, along with fat grafting can provide improvement in global volume or simply additional volume in areas of deficiency, such as the upper poles and medial cleavage region.
Key points
- •
Mastopexy, autoaugmentation, and fat grafting can be performed for primary breast correction without the use of an implant or in secondary surgery after explantation.
- •
Drawings are performed preoperatively as a guide with intraoperative adjustments expected.
- •
Ideal candidates for mastopexy with autoaugmentation have a high footprint, dense breast tissue, minor to moderate ptosis, adequate volume, and good quality skin.
- •
Vertical mastopexy with autoaugmentation is used with modest lifts and reductions, without excessive vertical excess, significant volume reduction, and/or when the nipple–areolar complex elevation is not more than 6 cm.
- •
The vertical mastopexy pedicle is superiorly based with parenchymal shaping through medial and lateral pillars; the skin excision design is often includes a vertical incision and removal of excessive vertical length through a horizontal wedge excision.
Introduction
Understanding the underlying cause of the ptosis, whether it be developmental or acquired secondary to weight loss, hormonal changes, pregnancy and/or aging, is critical in determining the appropriate surgical approach. In the initial assessment, it is important to determine the volume status of the breast, the extent of loss of upper pole volume, the quality of the breast tissue, and the patient’s goals for the procedure. The majority of mastopexy techniques focus on the elevation of the nipple–areolar complex (NAC) and the lower pole of the breast through skin tightening and potentially parenchymal resection. These techniques, however, have traditionally failed to establish and maintain volume in the upper pole in the long term. Patients desiring upper pole volume with breast ptosis often require the placement of an implant with the mastopexy to achieve the desired appearance. The addition of an implant to the procedure, an augmentation mastopexy, is by far the most popular and most successful method for achieving and maintaining upper pole volume after mastopexy.
However, there are many patients who will not accept the inclusion of breast implant but are dissatisfied with their breast shape and are seeking a mastopexy for improvement. There are also patients with implants in place with overlying ptosis who desire removal of the implants and a mastopexy. If it is determined that the volume of a breast implant is not necessary for the patient’s desired goal, the use of an autoaugmentation with or without fat grafting can optimize the results of a mastopexy in both primary and secondary breast lift procedures. There are a variety of mastopexy techniques described to address the ptotic breast. The techniques such as the circumareolar technique, circumvertical technique and inverted T scar technique. However, there is much more variation in the techniques, including the vascular pedicle orientation, management of the parenchyma and additional ancillary procedures to enhance the results. In an effort to optimize upper pole volume, various surgical techniques have been used, including parenchymal suturing techniques, local flap transpositions, and the use of a pectoralis sling for stabilization of the flap transfer. In our experience, the use of a lower pole parenchymal transposition flap to autoaugment the upper pole has been an excellent alternative. In primary cases, our approach most closely resembles that first described by Ribiero and more recently modified by Hammond. , This procedure is often combined with upper pole fat grafting to further enhance the outcome.
Perioperative decision making is critical to a successful outcome in an autoaugmentation mastopexy surgery. In this article, we review our approach to decision making with a focus on patient selection, review of mastopexy options, vascular anatomy of the transposition flap, and selection and planning of the mastopexy autoaugmentation procedure. The operative technique and postoperative care will be outlined in detail, providing a predictable approach that can produce the most successful outcomes, minimal complications, and very satisfied patients.
A decision on the appropriate mastopexy approach is based on not only the physical findings, but also patient expectations. In the preoperative evaluation, breast measurements, breast tissue density, quality of skin and breast parenchyma, NAC and breast ptosis, chest wall characteristics, and the breast footprint all must be considered in planning for the procedure. The ideal candidate would be a patient with adequate volume, a dense breast parenchyma, mild to moderate ptosis, good quality skin, and a high breast footprint ( Fig. 1 ). The upper pole flap transposition not only creates volume higher in the breast, it unloads the volume from the lower pole of the breast, potentially contributing to a more successful outcome as compared with a traditional mastopexy. Some patients present with low breast footprint, which can lead to unsatisfactory results if patient expectations were not discussed and outlined. It is difficult to change the low breast footprint without the addition of an implant or fat. Even if an implant is placed in such a patient, lower pole soft tissue support is needed for longevity results, given the inherent anatomy.

Blood supply and pedicle selection
An understanding and thorough assessment of the vascular anatomy is critical to performing the procedure safely. The breast has a rich blood supply from multiple sources, including the internal mammary artery (IMA) perforators, the lateral thoracic arteries, the thoracoacromial and the anterolateral and anteromedial intercostal perforators. The superior pedicle is supplied by the second branch of the IMA that emerges deep from the second interspace and courses superficial across the medial upper breast to enter the NAC slightly medial to the midline and approximately 1 cm deep. The superiomedial pedicle includes also the third branch of the IMA that emerges from the third interspace and similarly courses superficially across the breast parenchyma to the medial aspect of the NAC. The superficial position of these vessels in the upper pole allow the entire breast to be elevated off the muscle and chest wall in a subcutaneous plane for the planned flap transposition.
The central pedicle is supplied by the fourth branch of the IMA that courses deeply across the medial breast to enter through Wuringer’s septum approximately 1 to 2 cm above the inframammary fold (IMF) and often just medial to the breast meridian. This is the blood supply to the autoaugmentation flap in primary mastopexies ( Fig. 2 ). An understanding of the location of the fourth branch supplying this lower transposition flap is critical to creating a mobile flap of tissue with a viable pedicle blood supply. Obviously, if a patient has had a breast augmentation in the past or the breast has in any way been elevated off the chest wall previously, the central pedicle would have been divided and the flap transposition would not be possible. Thus, in patients undergoing explantation with a secondary mastopexy, the autoaugmentation flap is designed and based off of the blood supply feeding the NAC complex superior to the flap.
Primary mastopexy with autoaugmentation
Preoperative Evaluation
The evaluation should begin with a breast examination with breast measurements, including the base width, sternal notch to nipple distance, and nipple to fold distance (at rest and under maximal stretch). This assessment should also include an evaluation of the level of ptosis, the skin thickness and elasticity, the quantity and distribution of subcutaneous fat, the composition and firmness of the breast parenchyma, the integrity of the Cooper’s ligaments, the nature and position of the underlying musculature, and the shape and slope of the underlying chest wall. All these aspects of the breast composition influence the shape of the breast and ultimately the outcome after the mastopexy ( Box 1 ).
Relationship of the NAC to the IMF (Regnault’s degree of ptosis)
- a.
Grade 1: nipple at the level of the IMF, above the lower contour of the gland
- b.
Grade 2: nipple below the level of the IMF, above the lower contour of the gland
- c.
Grade 3: nipple below the level of the IMF, at the lower contour of the gland
- a.
Amount of breast tissue overhanging the fold
Location of the NAC on the breast mound
Amount of vertical excess and horizontal excess
Footprint of the breast on the chest wall – low, medium, or high
Quantity and quality of breast parenchyma and skin
One additional aspect in considering the mastopexy with autoaugmentation is the presence of an adequate amount of lower pole tissue to make the transposition possible and worthwhile. In patients with significant nipple descent but with short nipple–IMF distance, the vertical lower pole segment of tissue would be too short and inadequate to provide any benefit in the upper pole. Also, the footprint should be observed. Whereas this procedure can be performed on any footprint, it is the high breasted patient who benefits the most. In these patients, the short upper thorax requires only a small amount of tissue to produce a significant improvement. In the low-breasted footprint patient, the autoaugmentation does not elevate the upper breast border significantly enough and an implant would be a more appropriate option for correcting the upper pole. Most patients are not on either of these extremes, but more in the gray zone and judgment will be necessary. Likewise, assessing the firmness of the parenchyma is important, because patients with more firm, dense breasts do better at holding the shape in the long term compared with more lax breast tissue, such as a weight loss patient.
The mastopexy autoaugmentation is a circumvertical or vertical-type mastopexy and thus an assessment of the pedicle planned must be evaluated. The most common pedicle for this technique is a superior pedicle, but a superomedial pedicle is occasionally used. The medial pedicle is not generally used because the NAC is often located in the lower island segment of tissue and thus not available for use as an autoaugmentation. In our experience, elevation of the NAC on the breast superiorly beyond 5 to 6 cm, depending on the quality of the tissue, is less reliable with a superior pedicle and an inferior-based pedicle would be used and a mastopexy autoaugmentation would not be performed. This final judgment as to the viability of this technique is based solely on the surgeon’s comfort and experience in using a vertical approach with a superiorly based or superomedial blood supply ( Fig. 3 ). Because the flap uses the lower pole tissue, once the pedicle requires the use of the inferior flap tissue in the design, the autoaugmentation is not possible. The flap transposition to the upper pole is just a variant of the vertical mastopexy, and individual experience will determine the appropriateness of this approach.

Patient Expectations
One of the most critical elements of perioperative planning is patient education and understanding the patient’s desired outcome and expectations with the operation. Patients requiring a mastopexy have more significant changes to the breast than those needing simply a breast augmentation, and often have increased laxity of the tissue, stria, nipple and breast ptosis, and loss of parenchymal volume and/or firmness. Patients often are unaware of asymmetries, the significant atrophy of the breasts, and differences in the chest wall that affect the final outcome. During the evaluation, it is important to determine what “look” the patient would desire, especially in terms of nipple position and volume in the upper pole. Limitations must be discussed as to the results achieved with a mastopexy as compared with a breast augmentation or even an augmentation mastopexy. A patient desiring a more natural look and not requiring extremely full upper poles is an ideal candidate for this procedure. Sometimes patients are not always clear about the desired results and with the surge of social media posts, patients expectations have become more unrealistic. Patients need to understand that autoaugmentation with or without fat grafting does not achieve the same look as an implant. A mastopexy and autoaugmentation with or without fat grafting has limitations and can produce a only a somewhat fuller, naturally sloping upper pole at best. The procedure will not create the firm, full roundness that an implant can produce. These patients will also have scars on the breast, which at times can heal unpredictably, and a clear understanding of the location of the scars and anticipated outcome should be discussed.
Preoperative Markings
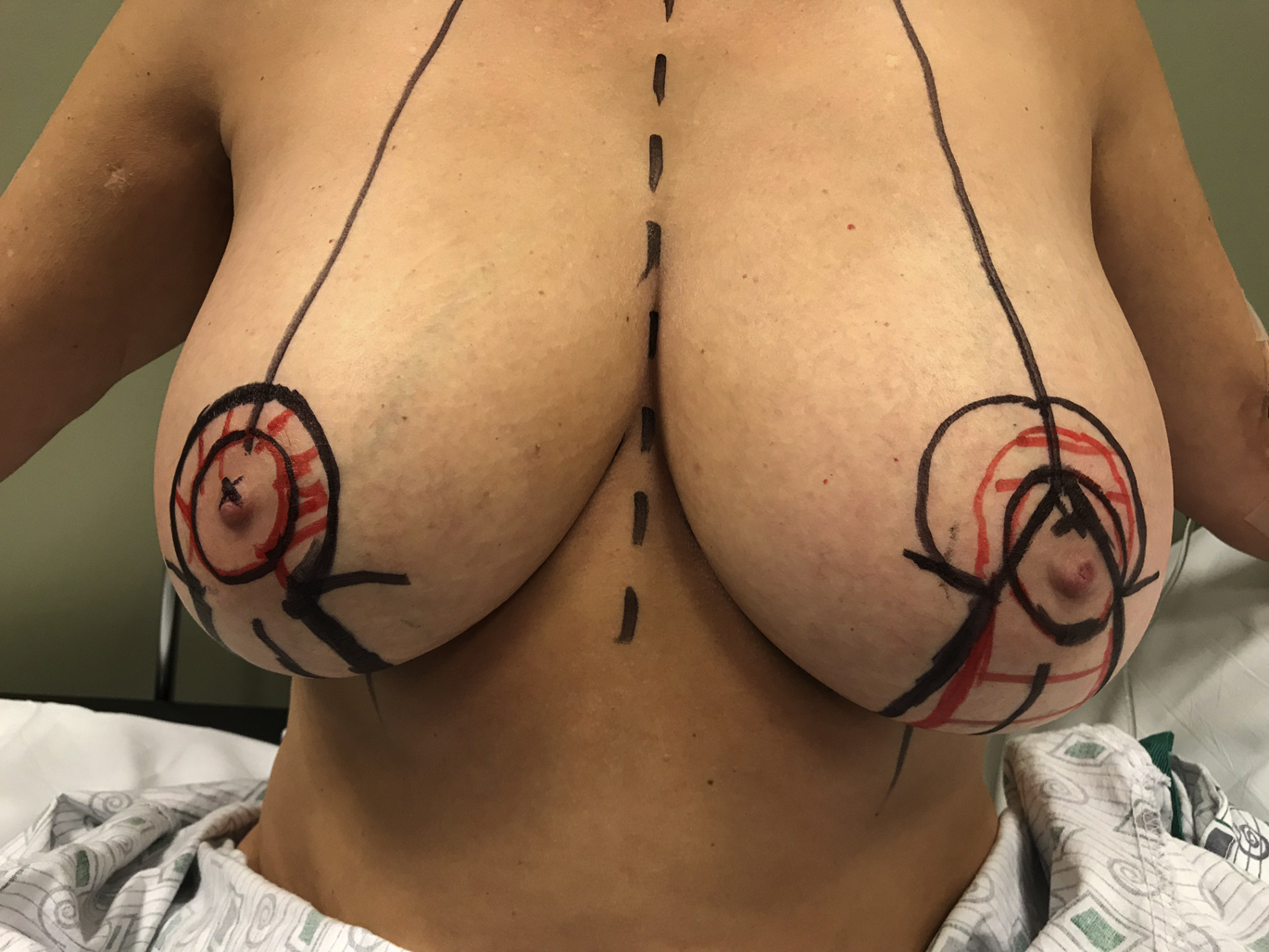
Appropriate preoperative markings guide the surgeon in providing symmetric NAC placement and mastopexy design. The patient is sitting upright during the markings. A line is initially drawn along the midline of the breasts and bilaterally down the meridians. The IMFs are then drawn, noting any asymmetries to be addressed at surgery. The position of the IMF is then drawn on the anterior breast through the meridian incision. The breasts are then rotated medially and laterally to mark the location of the vertical incisions.
This vertical mastopexy is based on a superior pedicle blood supply and is not dependent on the final skin excision pattern. The decision on nipple placement is made and is based on the location of the fold and expected location of the new lifted breast’s central mound position. This position can be approximated by simulating the mastopexy and identifying the probable location of the NAC. The nipple position is usually at or within 2 cm above the level of the reflected IMF, referred to as Pitanguy’s point. Placement of the areola is marked, starting approximately 2 cm above the nipple position and extending the curved drawing down to meet the medial and lateral vertical markings. This areolar opening marking should produce an areolar opening of approximately 42 mm. Approximately 6 to 7 cm below the bottom of the keyhole opening, a line is drawn marking the inferior extent of the vertical incision. Curved transverse lines are then drawn from these medial and lateral points extending down to the IMF. Approximately 2 to 3 cm above the fold, a U-shaped line connects the medial and lateral vertical markings to define the extent of skin resection ( Fig. 4 ).
Surgical Technique
The patient is placed on the operating room table with the arms secured to the sides at 45° to 60°. Once the patient is prepped with Chloraprep and draped appropriately, all markings are confirmed and retraced as necessary. The symmetry of the drawings is also confirmed. If any questions exist as to the accuracy of the markings, tailor tacking can be performed in many cases to reconfirm the markings. The tailor tacking should be adjusted as much as necessary to create the ideal breast shape. The superior pedicle is designed to be positioned in the superior keyhole from the 8 o’clock to 4 o’clock position. When in doubt about the mastopexy markings, it is advisable to stay conservative and leave a little more skin on the breast flaps. These parameters can be adjusted during the final assessment and contouring before the closure. The operative field is then injected with 50 mL per side of local anesthetic solution ( Table 1 ).
| Breast Local Anesthetic Formula | Volume |
|---|---|
| ½% Lidocaine plain | 25 mL |
| ½% Lidocaine/1:200,000 epinephrine | 25 mL |
| ½% Bupivacaine/1:200,000 epinephrine | 25 mL |
| Injectable saline | 25 mL |
| Total | |
| ¼% lidocaine, 1/8% bupivacaine, 1:400,000 epinephrine | 100 mL |
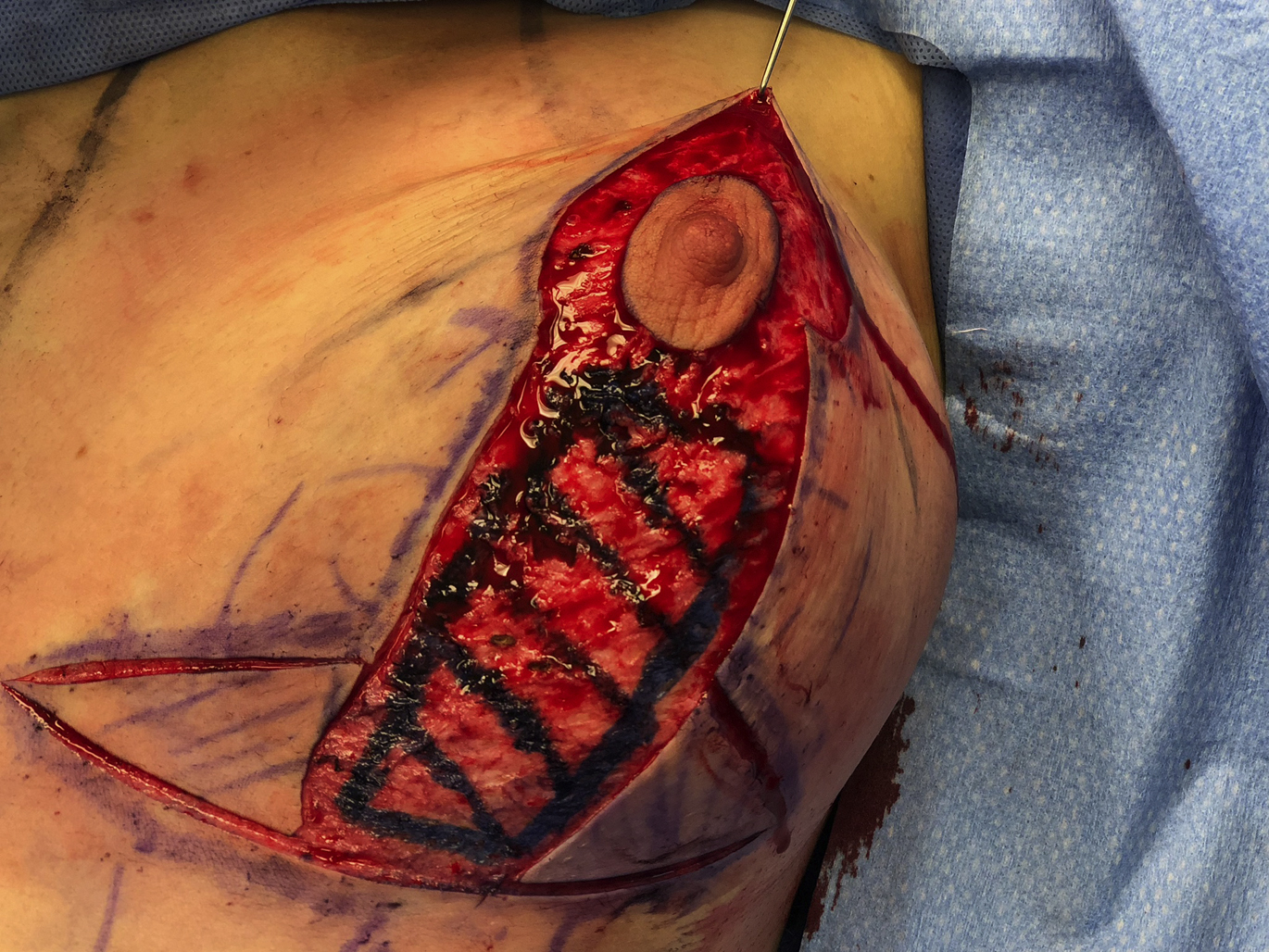
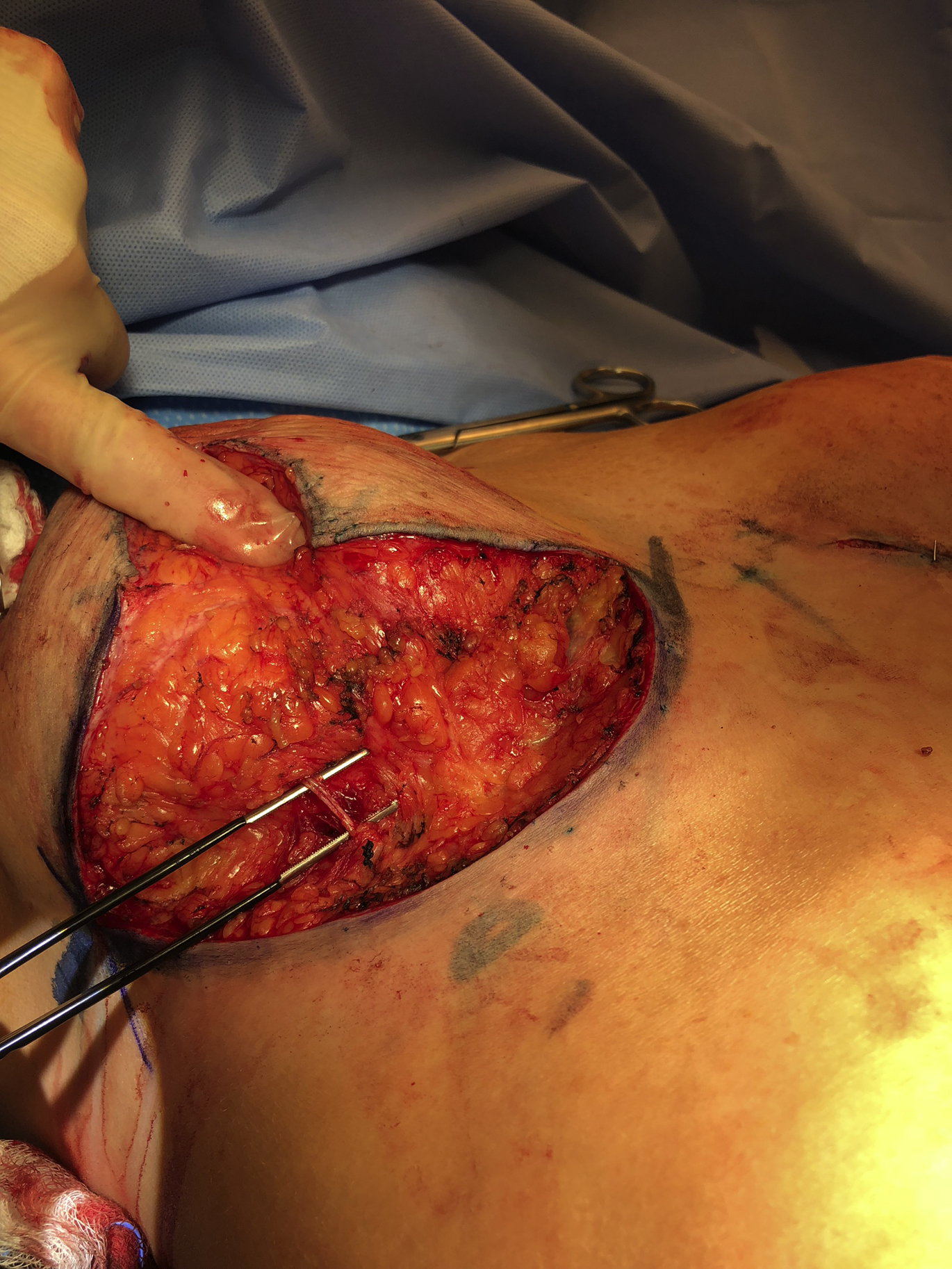
Each breast is then placed under maximal stretch and the areolas are marked with a 42-mm cookie cutter (range, 38–45 mm depending on the desired aesthetics) and incised. The entire area within the marks is then de-epithelized and cauterized for hemostasis and dermal shrinkage ( Fig. 5 ). The lateral and medial flaps are dissected straight down to the chest wall keeping them at least 2 cm thick. It is important to maintain good pillar volume to avoid lower pole deficiency ( Fig. 6 ).