This article discusses adjunctive skin care of the brow and periorbital region. Anatomic properties of eyelid skin require skin care products specifically suited to this area. Common patient concerns, including wrinkles, infraorbital dark circles, puffiness, and thinning eyebrows and eyelashes, are addressed in the context of contributing anatomic and physiologic factors and the classes of and/or specific ingredients targeting these problems.
Key points
- •
The unique anatomic characteristics of eyelid skin influence the types of skin care products suited to this area.
- •
Common concerns, including fine lines and wrinkles, infraorbital dark circles, under-eye puffiness, and thinning lashes and brows, can be treated by specific ingredients.
- •
Adjunctive skin care to treat the signs of photodamage may include sunscreen, topical antioxidants, retinoids, collagen boosters, and DNA repair enzymes.
- •
Knowledge of the contributing factors in the development of photodamage, dark circles and under-eye puffiness is needed to make skin care recommendations for these problems.
- •
It is important to set realistic patient expectations regarding the results of adjunctive skin care therapy.
Introduction
The periorbital region is often one of the first areas to show signs of aging and patients seek a dermatologist’s advice regarding care of the eyelid skin, often starting in their early 20s, well before seeking other antiaging treatments. In the context of a multidisciplinary approach to brow and eyelid rejuvenation, it is the dermatologist’s responsibility to be familiar with the many skin care options available for common concerns, including fine lines and wrinkles, infraorbital dark circles, and under-eye puffiness. Eyelid anatomy and aging are addressed in elsewhere in this issue by Lam and colleagues, Fitzgerald, Pepper and Moyer, Lee and Baker, Quatela and Lieberman, Day and Bucay, and Sundaram. They are also discussed in this article as they concern some key concepts relevant to understanding the aforementioned common complaints.
Introduction
The periorbital region is often one of the first areas to show signs of aging and patients seek a dermatologist’s advice regarding care of the eyelid skin, often starting in their early 20s, well before seeking other antiaging treatments. In the context of a multidisciplinary approach to brow and eyelid rejuvenation, it is the dermatologist’s responsibility to be familiar with the many skin care options available for common concerns, including fine lines and wrinkles, infraorbital dark circles, and under-eye puffiness. Eyelid anatomy and aging are addressed in elsewhere in this issue by Lam and colleagues, Fitzgerald, Pepper and Moyer, Lee and Baker, Quatela and Lieberman, Day and Bucay, and Sundaram. They are also discussed in this article as they concern some key concepts relevant to understanding the aforementioned common complaints.
Fine lines and wrinkles
Eyelid skin is the thinnest in the body, at times only 0.2 mm thick, contributing to its susceptibility to actinic and other damage. UV radiation is the primary cause of photodamage resulting in fine lines, mottled pigmentation, and textural changes. Other factors that lead to skin changes include genetic predisposition, smoking, and chronic rubbing due to seasonal allergies, irritants, or contact dermatitis. Components of adjunctive skin care to treat the signs of photodamage may include sunscreen, topical antioxidants, retinoids, collagen boosters, and DNA repair.
Sunscreens
Sunscreens are an indispensable element of adjunctive skin care of the eyelids and periorbital region. Classified as over-the-counter drugs, sunscreens should offer broad UV protection to include UVA (320–400 nm) and UVB (290–320 nm) and are integral in preventing UV immunosuppression. They should contain only ingredients that have been approved by the US Food and Drug Administration (FDA) as listed in the FDA’s Sunscreen Monograph Final Rule. Sunscreens are generally divided into two classes:
- 1.
Chemical—organic
- 2.
Physical—inorganic.
Chemical sunscreens (eg, benzophenone, homosalate, methyl anthranilate, octyl methoxycinnamate, oxybenzone, avobenzone) work by converting UVB radiation into heat, whereas physical sunscreens (eg, zinc oxide, titanium dioxide, kaolin, ichthammol, iron oxide) scatter, reflect and absorb solar radiation across a broad spectrum in the UV and visible ranges. In addition to their greater chemical stability, physical sunscreens have the added benefit of a minimal risk of contact sensitivity, an important consideration for delicate eyelid skin.
Topical Antioxidants
Topical antioxidants scavenge free radicals, which are highly unstable and reactive molecules. Free radicals that are generated from oxygen are known as reactive oxygen species. Capable of damaging cellular membranes, DNA, and cellular proteins, free radicals can be produced by normal cellular metabolism or can be triggered by external factors, including UV radiation and cigarette smoking. Skin aging is generally attributed to a combination of intrinsic and/or chronologic aging and extrinsic and/or environmental aging, and reactive oxygen species play a key role in both types of aging, a concept first published by Harman in 1956. Free radicals can also lead to inflammation, another factor that has been implicated in the aging process.
Vitamin C
Topical vitamin C (ascorbic acid) has been shown to reduce UV-induced erythema, sunburn cell formation, and the appearance of wrinkles. A combination of topically applied water soluble vitamin C (ascorbic acid), and a lipid soluble form, tetrahexyldecyl ascorbate (THD), has also been shown to reduce wrinkling due to photodamage. Studies have shown that, at the same concentration, THD surpasses the depth of penetration of ascorbic acid by threefold and that its rate of penetration is greater, even when the concentration of ascorbic acid is 25 times that of THD. Vitamin C plays an important role in collagen production and has been shown to stimulate collagen production when added to cultures of human skin fibroblasts. Vitamin C also restores the antioxidant capacity of vitamin E, a much more potent inhibitor of lipid peroxidation.
Vitamin E
Vitamin E is lipid soluble and consists of eight active isomers (tocopherols and tocotrienols), with alpha-tocopherol showing the most biologic activity. Vitamin E reduces the number of sunburn cells, decreases UVB-induced photodamage, and can inhibit UV-induced tumor formation. Alpha-tocopherol, a membrane-bound antioxidant, protects cell membranes from damage caused by phospholipase A, lysophospholipids, and free fatty acids. Vitamin E has been shown to inhibit human macrophage metalloelastase, a matrix metalloproteinase (MMP) that degrades elastin. Furthermore, signs of photoaging were shown to improve in a study comparing the use of a vitamin E cream versus placebo.
Combined vitamins C and E
The combined application of Vitamins E and C that is commercially available in several product lines has been shown to provide more potent photoprotection compared with either agent alone. A limitation to topically applied vitamin E is the potential for contact dermatitis.
Green tea
Green tea antioxidants extracted from the leaves and buds of the plant Camellia sinensis include epicatechin, epicatechin-3-gallate, epigallocatechin, and epigallocatechin-3-gallate (EGCG), the latter being the most abundant and potent. Animal studies have shown that topically applied green tea polyphenols can inhibit photocarcinogenesis as well as prevent UV-induced oxidative damage and induction of MMPs. In vivo application of green tea polyphenols to human backs 30 minutes before UV irradiation was shown to reduce erythema, the number of sunburn cells, immunosuppression, and DNA damage. Another study demonstrated the efficacy of topically applied EGCG in reducing UVB-induced inflammation. Although controlled clinical trials are lacking, green tea polyphenols are popular in cosmeceuticals given their ability to multitask. Vivian W. Bucay find them very helpful in mitigating the retinoid-induced irritation.
Vitamin B3
Topically applied niacinamide, the biologically active form of vitamin B3, not only exhibits antioxidant and antiinflammatory properties but also can improve hyperpigmentation by decreasing transfer of melanosomes to keratinocytes. The effects of topically applied niacinamide include improved skin texture and tone along with a reduction in fine lines and hyperpigmentation.
Side Effects of Topical Antioxidants
Side effects associated with topical antioxidants may include allergic contact dermatitis or irritant dermatitis. Topical vitamin E and niacinamide may induce allergic contact dermatitis, whereas irritant dermatitis may occur with some forms of topical vitamin C, such as the water-soluble forms, because higher concentrations are required for efficacy.
Retinoids
Retinoids are a classification of naturally occurring and synthetic compounds that exhibit the biologic actions of vitamin A. Their inclusion in countless antiaging products was triggered by Kligman and colleagues’ groundbreaking research on the effects of tretinoin on photodamaged skin in 1986.
Prescription retinoids
Of the prescription retinoids, only tretinoin and tazarotene have FDA approval for the treatment of photodamage, although nonprescription retinol and retinaldehyde are commonly used for this indication. Wrinkle improvement is the result of retinoid-mediated effects that produce an increase in dermal collagen synthesis by increasing type I procollagen expression mediated by the inhibition of the UV-induction of c-Jun and an alteration of transforming growth factor (TGF)-β expression. Inhibition of dermal collagen degradation is accomplished by inhibition of transcriptional factor activator protein-1 activation of MMP-like collagenase.
Retinoids also improve dyschromia by inhibiting tyrosinase activity. This leads to a reduction of melanin synthesis, decrease in melanosome transfer, and increase in shedding of keratinocytes. Additionally, retinoids contribute to smoother skin and a reduction in tactile roughness by increasing epidermal proliferation and differentiation, compacting the stratum corneum, and increasing epidermal and dermal intercellular mucin deposition.
Over-the-counter retinoids
Over-the-counter alternatives include retinol that, although potentially less irritating than its metabolite retinoic acid (tretinoin), is also 20-fold less potent. Retinaldehyde, a naturally occurring metabolite of retinol and the precursor of retinoic acid, has demonstrated efficacy in treating photodamage but with less irritation than retinoic acid. Eye skin care products containing hyaluronic acid, ceramides, cholesterol, and dimethylaminoethanol (DMAE) lactate are useful in mitigating dryness and skin irritation, and maintaining an adequate skin barrier.
Side Effects of with Retinoids
The most common side effect associated with retinoid use is an irritant dermatitis, characterized by excessive redness, dryness and flaking. This can be minimized by selecting the appropriate type of retinoid for the patient’s skin type, for example, retinoic acid or retinol for someone with thicker, oilier skin and retinaldehyde for those with thinner, drier skin. Additional strategies for mitigating skin irritation include decreasing the amount of product applied and/or the frequency of application. Layering the retinoid over a product containing antiinflammatory ingredients such as green tea polyphenols or coffeeberry also reduces skin irritation. Protective measures regarding sun exposure are strongly recommended and include sunscreen, sunglasses, and hats.
Patients should be counseled against using prescription retinoids during pregnancy and lactation. The authors recommend that each patient consult her obstetrician regarding the use of nonprescription retinoids during pregnancy and lactation.
Collagen Boosters: Peptides and Growth Factors
Peptides
Collagen boosters typically include compounds such as peptides and growth factors. A brief review of the pathogenesis of aging skin will aid in understanding the rationale for the use of these compounds in antiaging products:
- •
Lines and wrinkles occur both in photoaged and chronologically aged skin
- •
Coarser lines and wrinkles are characteristic of photoaging, whereas finer lines are more typical of chronologic aging
- •
The pathogenesis of skin aging is characterized by a decrease in collagen synthesis coupled with an increase in collagen breakdown
- •
A decrease in procollagen type I mRNA is seen in aging skin, with a greater reduction seen in photodamaged skin compared with nonexposed skin
- •
UV radiation–induced upregulation of collagenase (MMP-1) leads to damage and degradation of collagen.
Mechanisms by which an improvement in lines and wrinkles can be achieved include the upregulation of collagen production coupled with the down-regulation of collagen degradation, with dermal fibroblasts being the target cell in this strategy. To this end, peptides (short chains of amino acid sequences) have been incorporated into cosmeceuticals to stimulate collagen production. Peptides can be subdivided into three categories:
- 1.
Signal peptides
- 2.
Carrier peptides
- 3.
Neurotransmitter-inhibiting peptides.
Perhaps the most studied signal peptide is the five-amino-acid sequence Lys-Thr-Thr-Lys-Ser (KTTKS), which is found on type I procollagen and has been shown to increase the production of extracellular matrix proteins through the feedback regulation of collagen synthesis. Improved delivery of this hydrophilic peptide has been accomplished by adding palmitoyl, a 16-carbon fatty acid fragment, resulting in a compound known as Pal-KTTKS or, its commercial name, Matrixyl and is found in several commercially available products.
An example of a carrier peptide is the tripeptide glycyl-l-histidyl-l-lysine (GHK), which has been shown to facilitate copper uptake by cells and to stimulate fibroblast collagen synthesis. Additional effects of GHK include dermal remodeling by increasing levels of MMP-2 and MMP-2 mRNA and increasing levels of tissue inhibitors of metalloproteinase 1 and 2, increases in type I collagen and glycosaminoglycans, and increases in dermatan sulfate and cell layer-associated heparin sulfate.
In vitro studies have shown that acetyl hexapeptide-3, also known as argireline, functions as a neurotransmitter inhibiting peptide by interfering with sensory nerve action potential-25, thus mimicking the effects of clostridial botulinum neurotoxin. Although there is in vitro evidence of its ability to inhibit acetylcholine release, in vivo studies are limited, probably because of the inability of this compound to penetrate to the muscle. Nonetheless, argireline has been incorporated into several cosmeceutical products.
Additional peptides include tripeptide-1 (Aldenine), which acts by reducing glycation and advanced glycation end products by increasing superoxide dismutase and decreases collagen cross-linking and other peptides, and palmitoyl tetrapetide-7 and palmitoyl oligopeptide (together known as Matrixyl 3000), which act to stimulate type I collagen, fibronectin, and hyaluronic acid. Additional peptides will be covered under the topic of puffiness and dark circles.
Growth factors
Growth factors are high molecular weight peptides that regulate specific cellular activities, including tissue repair and growth and intercellular signaling. There is evidence to suggest that the following play a role in skin rejuvenation :
- •
TGF
- •
Epidermal growth factor
- •
Platelet-derived growth factor
- •
Insulin-like growth factor
- •
Fibroblast growth factor
- •
Vascular endothelial growth factor (VEGF).
A double-blind study involving 60 subjects examined the safety and efficacy of a proprietary mixture of more than 110 growth factors, cytokines, and soluble matrix proteins secreted by human fibroblasts in the treatment of mild to severe photodamage. Patients were randomized to receive either the active gel or the vehicle and were instructed to apply it twice daily. Both subjective and objective measurements at 3 months showed a greater reduction in fine lines and wrinkles by the active gel when compared with the vehicle, suggesting that a topical gel of growth factors and cytokines can improve the signs of photoaging when used with a sunscreen.
Alternatives to human growth factors are those derived from plants, such as N-furfuryladenine, and animal-derived growth factors, such as snail secretion filtrate, the most biologically active of which is derived from Cryptomphalus aspersa (SCA). This compound has been used successfully in Europe for over 15 years to treat radiation dermatitis. SCA is found in commercially available products used to treat the signs of photoaging and at least one published study has demonstrated its efficacy in the treatment of periocular wrinkles.
DNA repair liposomes have been shown to reduce the incidence of UV-induced skin cancer in mice, although to date, there are no controlled clinical studies in humans demonstrating the same. Despite the lack of clinical studies, incorporation of these compounds into antiaging products is becoming increasingly popular, and the author is aware of some ongoing studies involving some of the commercially available products.
DNA repair enzymes include photosomes, which are a plankton-derived form of photolyase and block the transcription of UV-induced pyrimidine dimers, roxisomes or oxoguanine glycosylase-1; a mitochondrial DNA repair enzyme obtained from the Arabidopsis thaliana (mustard) plant, which serves to excise damaged DNA; and ultrasomes, or T4 endonuclease, which is derived from Micrococcus lysate and acts by excising UV-induced dimers. Liposomal formulation of these enzymes allows for targeted delivery and enhanced efficacy. Photobiologist and cosmeceutical innovator Daniel Yarosh, PhD, has published more than 100 articles on the subject of DNA repair; his book, The New Science of Perfect Skin , is an excellent reference on the science of skin care.
Stem cells are a hot topic in many areas of medicine and their incorporation into skin care is an emerging trend. Plant stem cells, such as apple stem cells, can be found in currently available skin care products; however, the inclusion of autologous human cells in skin care heralds the latest advance in the treatment of photodamage. An additional application of the recent FDA approval of technology involving the injection of an autologous fibroblast suspension for the treatment of fine lines and wrinkles will extend to the use of these same cells to formulate personalized skin care. Controlled clinical trials will be necessary to prove their efficacy.
Complications with Peptides and Growth Factors
A theoretical complication associated with the use of human growth factors is the development of skin cancers or the progression of precancerous lesions to skin cancer in susceptible or predisposed individuals. Vivian W. Bucay emphasize that the potential for skin cancer is theoretical and based on personal experience (the development of actinic keratoses and/or squamous cell skin cancer in one author and four others following use of a cosmeceutical containing VEGF) and that there are no reports in the literature documenting the development of skin cancer associated with cosmeceutical use.
This discussion is limited to VEGF and its effect on skin cancer development because there are ample references in the literature regarding the subject. Research shows that levels of VEGF are at least 10 times higher in patients with melanoma. Melanoma cells express receptors for various growth factors, such as VEGF, and increased angiogenesis secondary to excessive VEGF exposure has been shown to be a fundamental step in the transition of dormant tumors to malignancies. The role of VEGF in melanoma is discussed because melanoma is the deadliest form of skin cancer, although not the most common. Squamous cell carcinoma is the second most common skin cancer, and important progress regarding the role of VEGF in tumor initiation and progression has been made. Cancer stem cells have been described in several cancers, including cutaneous squamous cell tumors. Through work on defining the mechanism of action of VEGF-targeted therapies, it is known that VEGF exerts its effects on tumors not only through angiogenesis but also via a direct effect on tumor cells. Using a mouse model for squamous cell tumors (considered ideal for studying skin cancer initiation and growth ), Beck and colleagues delineated the dual role of VEGF in regulating the initiation and stemness (the ability of cancer stem cells to renew and differentiate themselves). They showed that VEGF promotes cancer stemness and symmetric cancer stem cell division via neurolipin-1 (Nrp1), a VEGF coreceptor expressed in cutaneous cancer stem cells and the deletion of Nrp1 in normal epidermis prevented skin tumor initiation.
VEGF is upregulated by UVB exposure from sunlight, adding to the susceptibility of unprotected skin. Patients are often reluctant to apply sunscreen to the eyelids and periorbital region, citing such reasons as burning, stinging, and tearing of the eye area. It is the authors’ opinion that, although cosmeceutical products containing human growth factors are not subject to the same testing and FDA regulations as prescription drugs are, there is still much to be learned and understood regarding their mechanism of action and caution should be exercised when used in patients with a high risk or history of skin cancer.
Infraorbital dark circles and puffiness
Compared with the extensive research that contributes to our understanding regarding the mechanisms that lead to photoaging, there is a relative paucity of scientific information regarding the causes of under-eye puffiness and dark circles, which cannot be studied via animal models and tissue cultures. For this reason, the underlying causes of these common complaints are discussed here in terms of contributing anatomic and physiologic considerations.
Although not a condition associated with morbidity, dark circles are often a source of cosmetic concern that can have a negative impact on an individual’s quality of life because they can convey a sense of sadness or fatigue, even when these are not the case. Causes of dark circles are numerous and usually not limited to a single factor in a given individual and include excessive pigmentation, thin and translucent eyelid skin, shadowing secondary to skin laxity, and anatomic age-related changes leading to hollowing and tear trough deformity.
Excessive Pigmentation
Excessive pigmentation may be caused by underlying dermal melanocytosis, which may also be attributed to congenital causes, such as nevus of Ota, sun exposure, drug ingestion, or medical conditions including atopic or contact dermatitis that leads to rubbing or scratching of the periorbital region with the development of postinflammatory hyperpigmentation. Hemosiderin deposition due to “leaky” vasculature or following trauma may also cause pigmentary changes in the lower eyelids. Depending on the underlying cause and the depth of pigmentation, treatment options may include topical prescription medications to treat an underlying medical problem, laser modalities, chemical peels, and/or cosmeceutical agents.
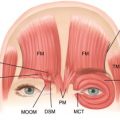
As already mentioned, the eyelids have the thinnest skin of the body, and the orbicularis oculi muscle lies just beneath the eyelid skin with minimal subcutaneous fat found between the muscle and skin. This is a contributing factor to the appearance of dark circles. A prominent subcutaneous and/or muscular vascular plexus will result in a violaceous hue under the eyes that does not blanch but deepens in color with manual stretching of the skin. This maneuver of stretching the skin to produce deepening of the violaceous color may serve as useful diagnostic tool to confirm the vascular cause of the pigmentation. Moreover, in their review on this subject, Roh and Chung state that the successful use of autologous fat transplantation to reduce the appearance of hypervascularity supports the idea that it is the vasculature found within the muscle instead of the combination of thin skin and subcutaneous vascularity that plays a greater role in the appearance of these violaceous infraorbital dark circles.
In addition to autologous fat transplantation, various modalities, including laser and other energy-based devices as well as soft tissue fillers, have been tried with varying success. In keeping with the theme of adjunctive skin care of the eyelids, topical agents that exert effects on the vasculature will be discussed, although, as is the case with many cosmeceuticals, controlled clinical studies to support their use are lacking.
Shadowing
Shadowing due to intrinsic and extrinsic aging of the skin that leads to skin laxity, in combination with age-related changes in the soft tissue and skeleton, is another common cause of dark circles. The appearance of a “tear trough” depression secondary to loss of subcutaneous fat and thinning of the skin over the orbital rim ligament leads to hollowing of the orbital rim, leading to a dark shadow that can be further accentuated by pseudoherniation of the infraorbital fat pad. Short of addressing the issue of photodamaged skin as discussed earlier in this article, adjunctive skin care does not play a role in the treatment of this type of infraorbital dark circle.
Puffiness and bags
Under-eye puffiness and lower eyelid bags are also multifactorial in origin and another common aesthetic complaint, although published studies regarding this topic are scarce. In an analysis of 114 consecutive subjects (67 men and 47 women, mean age 52 years, age range 23–76 years) presenting for aesthetic consultation for lower eyelid bags, Goldman and colleagues conclude that there is not a single anatomic basis for their cause but, instead, identify six anatomic variables. These include
- 1.
Cheek descent and hollow tear trough (52%)
- 2.
Prolapsed of orbital fat (48%)
- 3.
Skin laxity and sun damage (35%)
- 4.
Eyelid fluid (32%)
- 5.
Orbicularis hyperactivity (20%)
- 6.
Triangular cheek festoon (13%).
Not surprising, tear trough depression, skin laxity, and triangular malar mound occurred with greater frequency in those older than 50 years, and linear regression analysis showed that a recommendation for surgery was based on the extent of fat prolapse, skin elasticity, and midface descent.
Surgical intervention, laser resurfacing, soft tissue fillers, neurotoxins, and energy-based skin tightening may be used in varying combinations to address this complaint. Nonetheless, despite the evidence in support of an anatomic basis for under-eye puffiness and bags, patients seek recommendations for cosmeceuticals that can diminish their appearance. Most products used for this indication contain ingredients to reduce fluid retention, strengthen the vasculature, and improve skin laxity.
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


