Fig. 1.1
A keratotic nodule with erythematous halo on the scalp of an old patient
Pathology
Histologically, the tumor is composed of cords and nests of atypical keratinocytes with an infiltrative pattern of growth. Connection to the overlying epidermis, which may show hyperkeratosis and parakeratosis, is present in most cases, even if sometimes it may be only focal or absent (Fig. 1.2). Many of the tumor cells may show tubular, alveolar, and pseudoglandular arrangement. The hallmark of the lesion is the pseudogland, which is an open space lined by atypical flat, cuboidal, or cylindrical cells (Fig. 1.3). The space usually contains isolated acantholytic necrotic cells floating within the lumen (Fig. 1.4). The epithelial cells are atypical with bright eosinophilic, focally glassy cytoplasm arranged in loose cohesive clusters representing pseudoacantholysis (Fig. 1.5). ASCC stains positively for immunohistochemical markers towards pankeratin and epithelial membrane antigen (EMA), but immunostains for carcinoembryonic antigen (CEA) give invariably negative results. In the literature, a decreased expression of intercellular adhesion proteins, such as of Dsg3, E-cadherin, and syndecan-1, has been described in ASCC compared to conventional SCC, and it has been suggested that this may contribute to the development of acantholysis and of the controversially more aggressive biological behavior.
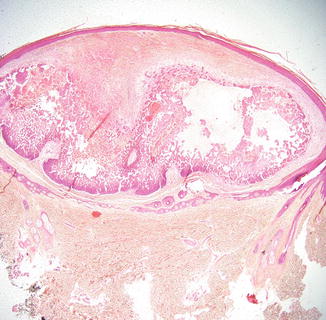
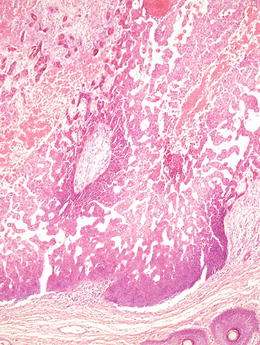
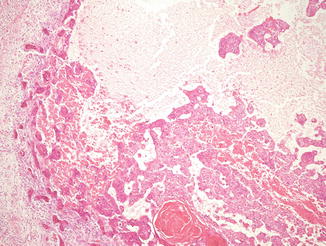
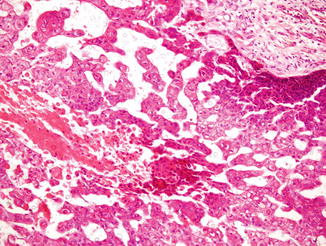
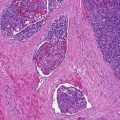
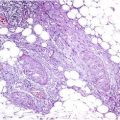
Fig. 1.2
A squamous tumor extending into the dermis with pseudoglandular spaces and necrotic areas
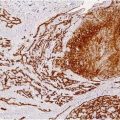
Fig. 1.3
Pseudovascular or pseudoglandular appearance due to tumor cell discohesiveness and necrosis
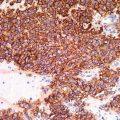
Fig. 1.4
Lining is composed of squamous epithelium and spaces with necrotic debris, keratin, and keratinous cyst
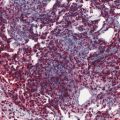
Fig. 1.5




The epithelial cells are atypical with bright eosinophilic, focally glassy cytoplasm arranged in loose cohesive clusters representing pseudoacantholysis
Related posts:

Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
