Addressing Late Malpositioning of the Zygomaticomaxillary Complex
Warren Schubert
Yeshaswini Thelekkat
DEFINITION
Late malpositions of the zygomaticomaxillary complex (ZMC) result when fractures either were not addressed at the time of the original trauma or were opened and internally fixated but not properly reduced.
The term late in this chapter refers to fractures that have healed in a malposition and require an osteotomy to mobilize and reposition the zygoma.
The term OIF (opened and internally fixated, but not reduced) has been popularized by Joseph Gruss to suggest that rather than have a proper ORIF (open reduction and internal fixation) the patients have been opened and internally fixated but not properly reduced, resulting in a malposition of the ZMC.
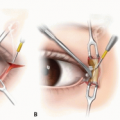
The authors have been impressed that elderly and malnourished patients with ZMC fractures—even 6 weeks after initial trauma—can occasionally be replicated and mobilized using an osteotome without a saw and then fixated using methods outlined in the chapter on primary fixation of acute ZMC fractures.
Osteotomies in a potentially new plane should always be avoided if the exact positions of the previous fractures can be replicated.
ANATOMY
The key is attaining proper repositioning and stabilization of the zygomatic processes and buttresses.
Though not absolutely required, the surgeon may consider a coronal approach when addressing a late malposition. As a result, a plate on the zygomatic arch to restore the AP position of the zygoma is more likely to be considered when addressing a late malposition than in routine acute ZMC fractures.
The goal is to re-establish the alignment and proper position of the zygomaticofrontal (ZF) fracture, the lateral wall of the orbit (junction between the greater wing of the sphenoid and the zygoma), the orbital floor, the inferior orbital rim, the lateral maxillary column of the midface, and the zygomatic arch (FIG 1).
PATIENT HISTORY AND PHYSICAL FINDINGS
The patient may present with a variety of deformities including blunting of the malar eminence, enophthalmos, diplopia, dystopia of the eye, lateral canthal malposition, widening of the midface or depression of the zygomatic arch, and numbness in the infraorbital nerve distribution.
IMAGING
As with an acute ZMC fracture, the appropriate radiologic workup requires fine-cut computed tomography (CT) slices.
The ideal workup includes axial cuts, reformatted coronal cuts, and oblique parasagittal cuts through the orbit. 3D reformatting of the midface may also be useful (FIG 2).
Because the surgeon is faced with issues of remodeling of the bony fragments, exact repositioning of the osteotomized segments may present a challenge.
The surgeon may choose to use intraoperative CT to ensure the proper reduction of the osteotomized segments in the same way that surgeons have used this technique for acute fractures.1
Navigation may be used intraoperatively in a similar way that intraoperative imaging is used if this technology is available to the surgeon.2
With navigation, obtaining a preoperative CT with a fiducial guide may be necessary.
The surgeon is able to perform a virtual correction of the proper placement of the ZMC on the injured side by mirroring the proper position of the ZMC from the contralateral uninjured side.
At the time of surgery, the malpositioned ZMC is moved into its proper position as visualized in the virtual image.
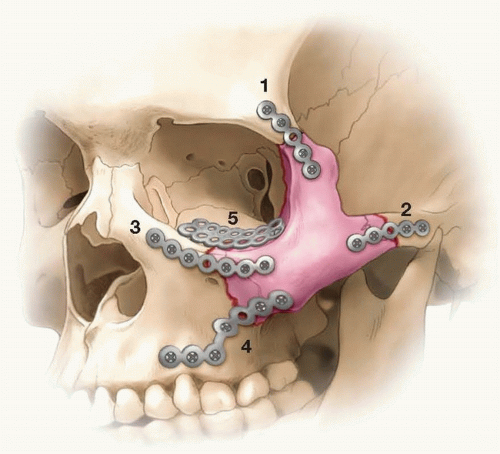 FIG 1 • Key anatomic points that need to be realigned and fixated: (1) Fronto-zygomatic suture; (2) Zygomatic arch; (3) Infraorbital rim; (4) Zygomatico-maxillary buttress; (5) Orbital floor. |
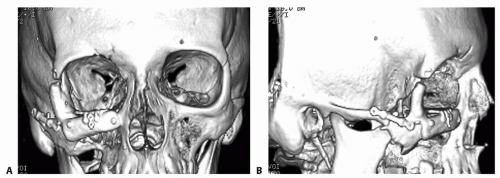 FIG 2 • A. AP CT of a late malposition of the ZMC in a patient who has had multiple past procedures, including a bone graft of the inferior orbital rim. It is clear that the ZMC was fixated without reduction (OIF). B. Lateral CT shows that a proper reduction of the ZF suture and the zygomatic arch was never achieved. |
NONOPERATIVE MANAGEMENT
Nonoperative management is always an option.
The authors’ only experience with blindness with a ZMC repositioning occurred after an osteotomy was performed for correction of a late malposition. Our impression is that addressing a chronic deformity with enophthalmos has a significantly higher associated risk of blindness, possibly due to an orbital compartment syndrome, than does repositioning of an acute ZMC fracture.
SURGICAL MANAGEMENT
Preoperative Planning
A complete ophthalmic examination should be performed by documenting the canthal and lid positions, identifying if there is a superior sunken sulcus of the upper eyelid, full movement of the extraocular muscles, diplopia, dystopia, and field defects.
Exophthalmometric measurements of the degree of enophthalmos may be useful.
As the lateral aperture of the orbit is often displaced, we prefer using a Naugle exophthalmometer over a Hertel and resting the Naugle on the frontal bar (FIG 3A). This assumes that the fractures being addressed do not include a displaced frontal bar.
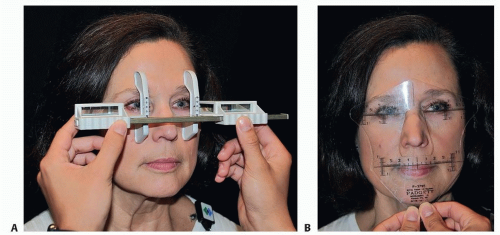
FIG 3 • A. Demonstration of a Naugle exophthalmometer for measuring globe protrusion. The advantage of this exophthalmometer is that unlike the Hertel, it does not rest on the lateral orbital aperture. If the malar eminence is involved with the trauma, it is possible to slightly tip the device up so that it is resting on the frontal bar. Though the absolute measurements may be slightly distorted, the surgeon is able to gain a good idea of the relative degree of globe protrusion (or enophthalmos) compared to the uninjured side. B. Demonstration of the use of the McCoy facial trisquare to examine the relative position of the medial and lateral canthus.Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree

 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access