Acute Vascular Injuries of the Upper Extremity
James P. Higgins
Penetrating trauma accounts for over 80% of the acute arterial injuries to the upper extremity. Blunt trauma, closed fractures, or thermal injuries can also produce acute arterial injuries. Regardless of the etiology, accurate, rapid assessment and treatment of these problems require a thorough understanding of the detailed arterial anatomy of the upper extremity with a focus on both major vessels and sources of collateral perfusion.
I. Anatomy
Left subclavian artery originates from the aortic arch. Right subclavian and right common carotid arteries originate from brachiocephalic trunk.
Clavicle is landmark for the transition of vessel name from subclavian to axillary artery.
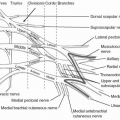
Axillary artery passes deep to the pectoralis major and minor, intimately enveloped by the infraclavicular brachial plexus.
Axillary artery is the source of several branches to the shoulder and thorax:
Thoracoacromial artery
Lateral thoracic artery
Subscapular trunk (thoracodorsal and circumflex scapular arteries) Inferior margin of pectoralis minor muscle is landmark for the transition of vessel name to brachial artery.
Brachial artery courses anterior to the intermuscular septum of the medial brachium, initially running between the median nerve (anterior to the artery) and the ulnar nerve (posterior to the artery). In the distal portion of the upper arm, the median nerve passes medial to the brachial artery as they approach the antecubital fossa.
The brachial artery supplies three major sources of collateral flow across the elbow:
Deep brachial artery—passing posterior and lateral to the humerus in tandem with the radial nerve to join the radial artery distally.
Superior ulnar collateral artery—passing posterior to the medial epicondyle in tandem with the ulnar nerve to join the ulnar artery distally.
Inferior ulnar collateral artery—passing anterior to the medial epicondyle to join the ulnar artery distally.
The brachial artery bifurcates in the antecubital fossa to form the radial and ulnar arteries.
Radial artery courses more superficially than the ulnar artery in the proximal forearm, coursing deep to the bicipital aponeurosis and brachioradialis, and superficial to the biceps tendon, pronator teres, FDS, and FPL sequentially. At the wrist, it can be located between the brachioradialis and FCR tendons.
At the wrist, the radial artery bifurcates into a smaller volar branch and a larger dorsal branch.
Volar branch passes superficial or within the APB to join the superficial palmar arch
Dorsal branch courses deep to the first dorsal extensor tendon compartment into the anatomic snuffbox and divides into two major branches.
The first creates the dorsal arch of the hand.
The second passes between the first and second metacarpal bases to supply the deep palmar arch distally.
The “princeps pollicis” artery to the thumb branches off the radial artery in this region. Variability in its origin is encountered frequently.
Ulnar artery courses deeper in the forearm after branching from the brachial artery, coursing deep to the pronator teres, median nerve, and FDS. Shortly after its departure from the brachial artery, the ulnar artery serves as the source of the common interosseous artery. The ulnar artery then migrates ulnarward along the superficial surface of the FDP to join the ulnar nerve at the junction of the middle and distal thirds of the forearm. The ulnar artery and nerve pass through the distal aspect of the forearm in tandem. At the wrist, the ulnar artery can be located deep and radial to the FCU tendon, and radial and superficial to the ulnar nerve at the wrist. At the wrist, the ulnar artery passes into Guyon canal, where it bifurcates. The larger superficial branch supplies the superficial palmar arch. The smaller deeper branch (coursing in tandem with the motor branch of the ulnar nerve) joins the deep palmar arch.
Common interosseous artery branches off the radial aspect of the proximal ulnar artery. It divides into anterior and posterior branches.
The anterior interosseous artery travels in tandem with the anterior interosseous nerve along the volar surface of the forearm interosseous membrane (IOM).
The posterior interosseous artery courses through a fenestration in the IOM and enters the dorsal compartment. It is found deep to the EDC and EDQ muscles and superficial to the more obliquely oriented APB, EPB, EPL, and EIP muscle bellies. Cutaneous perforators are found roughly at the junction of the proximal third and distal two thirds.
At the wrist, the anterior and posterior interosseous arteries communicate a second time via the posterior division of the anterior interosseous artery that passes through a fenestration in the IOM. Both volar and dorsal components create a rich network of communicating vessels at the radiocarpal level, creating small arcades designated palmar metaphyseal arch, palmar radiocarpal arch, dorsal supraretinacular arch, dorsal radiocarpal arch, and dorsal intercarpal arch. These are clinically significant in two ways:
They are the source vessels of an expanding number of pedicled bone grafts for the treatment of carpal pathology (fracture, nonunion, AVN).
They supply routes of collateral flow in the setting of injury to large vessels of the forearm.
Superficial palmar arch—Supplied by the superficial branch of the radial artery and the superficial (dominant) branch of the ulnar artery. Creates an arcade deep to the palmar fascia and superficial to the median nerve and flexor tendons. This arcade is the source of common digital arteries to web space 2 to 4, as well as ulnar digital artery to small finger. These common digital arteries run in tandem with the common digital nerves. The arteries bifurcate into proper digital
arteries designated by the aspect of the digit they supply (i.e., “ulnar digital artery to ring finger”). The common digital nerves bifurcate more proximally in the palm and migrate palmarly. The digital nerves are thus deep to the arteries in the palm and superficial to the arteries in the digit.
Deep palmar arch—Supplied by the dorsal branch of the radial artery after it passes from the snuffbox in the dorsum of the hand, between the bases of metacarpal 1 and 2, into the palmar space. This arch runs transversely at the level of the metacarpal bases. It supplies the palmar metacarpal arteries that lie deep to the flexor tendons and neurovascular structures. Palmar metacarpal arteries communicate with digital arteries through communicating perforators at the level of base and neck of the metacarpals. The deep palmar arch typically supplies the digital arteries to the thumb and the radial digital artery to the index finger. There is significant anatomic variation seen in this region of the first web space. The term “princeps pollicis artery” has been employed to describe many different anatomic structures, which serve as the main blood to the thumb. The use of this term should be avoided because of this lack of agreement on its definition.
Dorsal arch (AKA Dorsal Intercarpal Arch)—Supplied by the dorsal branch of the radial artery. This supplies the dorsal metacarpal arteries and feeds into the rich plexus of dorsal wrist small vessel connections to the interosseous arteries (see F). Dorsal metacarpal vessels course along the fascia of the dorsal interosseous muscles and feed angiosomes out to the level of the PIPJ of digits 2 to 5 and out to the tip of the thumb. These vessels can routinely maintain viability of the entire thumb despite injury to both digital arteries of the thumb. They cannot reliably maintain viability of the remaining digits after similar injuries to their respective digital vessels.
Proper digital arteries
Course dorsal (deep) to digital nerves, but volar to the midaxis of the digit.
Can be found dorsal to Grayson ligaments and volar to Cleland ligaments
One digital artery can maintain viability of the entire digit after single digital artery injury. This is due to rich arcades of communicating volar vessels located between the palmodigital and IP flexion creases.
An isolated injury to a common digital artery will not result in critical ischemia of a digit. This is due to the anatomic relationship of the common digital arteries supplying proper digital arteries to adjacent fingers.
The dominant artery for the index and middle fingers is usually the ulnar digital artery, and the dominant artery for the ring and the small fingers is usually the radial digital artery.
II. Diagnosis
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


