Acute Burn Injury

Description
Flame burn injury to portions of the face, the left chest, and left arm.
Superficial and deep partial-thickness burns.
Approximately 20% of body surface area.
Possible circumferential involvement of the forearms.
Concern for inhalational injury.
Work-up
History and physical examination
Trauma evaluation
ABCs (airway, breathing, circulation): Assess for critical injuries during the primary survey.
Mechanism of injury
Flame: Most common. Can lead to superficial to deep burn, depending on degree of exposure.
Oil or grease burns: Must be careful not to underestimate severity of such burns. Oil will continue to burn over lengthy periods of time if not washed off immediately.
Electrical (high or low voltage): Raises concern for deeper injury to the underlying structures. Greater concern for compartment syndrome and rhabdomyolysis.
Enclosed versus open space: Enclosed locations increase likelihood of inhalational injury.
Inhalation injury
Examine for singed facial hair, soot in airway.
History of asthma or chronic obstructive pulmonary disease (COPD) can compromise oxygenation.
Any significant concern warrants intubation.
Extent of burn
Rule of nines (Fig. 39.2): Calculation of extent based on second- and third-degree burns. Does not include first-degree burns.
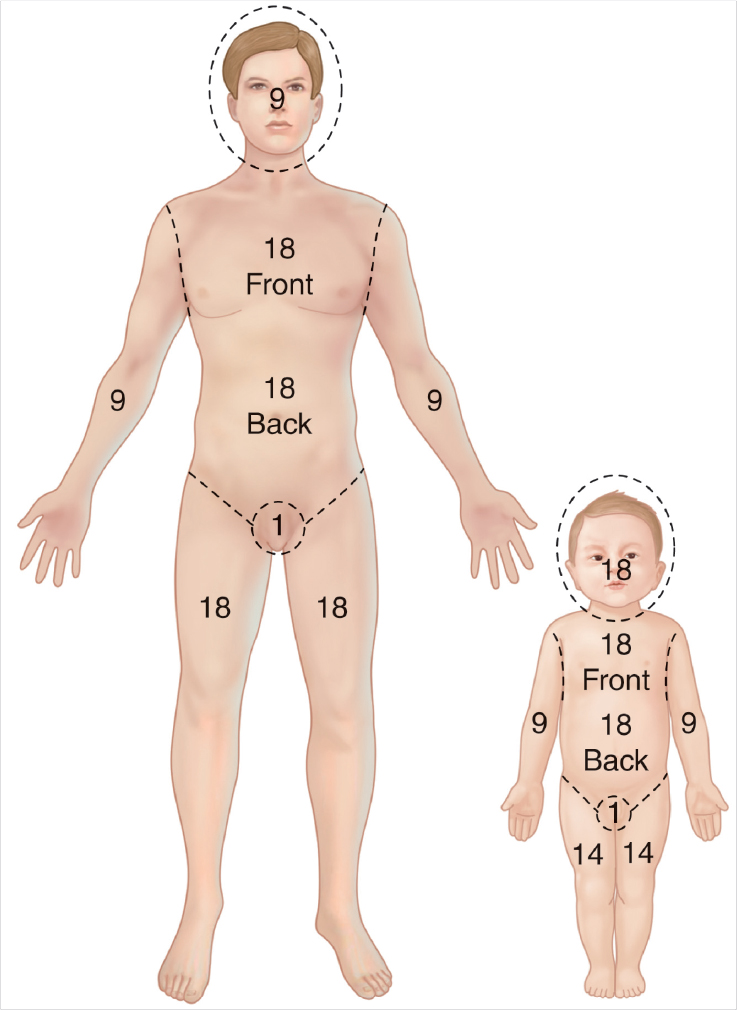
Rule of nine for estimation of burn injury. Note the increase in proportion of the size of the head in children.
Assess depth of burn: Partial (superficial or deep) versus full thickness.
If electrical: Identify entrance and exit wounds to determine path of injury.
Extremities involved
Circumferential burns: Assess need for escharotomies or fasciotomies.
Compartment syndrome (see Case 40)
Compartmental pressures may be measured with STIC pressure monitor (Stryker; Kalamazoo, MI).
Concern if pressures > 30 mm Hg.
Assess distal perfusion.
Face involved
Eyes: consider ophthalmology consult.
Cartilage exposure: Assess for presence of exposed tissues.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


