Hand Burn

Description
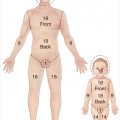
Noncircumferential second- and third-degree burns to the upper extremity.
Dorsal hand and fingers involved.
No significant palmar burns present (not shown in photograph).
Neurovascular status is intact distally.
Work-up
History
Age, gender, handedness, and occupation of the patient.
Timing and mechanism of burn injury
Thermal: Type of burn (flame, contact, scald, steam, grease); duration of contact; associated injury; tetanus status; suspicion of abuse.
Chemical: Type of chemical (alkali, acid, organic compound); duration of contact; neutralization attempted.
Electrical: Type of current (AC or DC), voltage, duration of contact, pathway of current flow.
Previous injury or surgery to the hand in question.
Manual demands of daily living and overall lifestyle.
Past medical and surgical history.
Medications and allergies.
Social history, including smoking status and substance abuse.
Physical examination
Initial assessment of hand burns pertains to vascular perfusion and to the depth and distribution of the burn injury.
Hand is scrubbed of any soot, dirt, or debris.
Potentially constricting jewelry and watches are removed.
Acute injury
Location and total surface area of burn injury.
Depth of burn injury (first-degree, superficial second-degree, deep second-degree, third degree).
Exposure of deep structures (e.g., tendons, bones, neurovascular structures).
Vascular status of hand.
Motor and sensory function.
Compartment syndrome: Limb-threatening condition
Mostly seen in combined crush or other significant injury (otherwise see notation on eschartomy below, which is more pertinent to isolated burn mechanisms of injury).
High index of suspicion necessary.
Pain out of proportion to injury, especially with movement.
Five P′s (late signs): pain, pallor, paresthesias, paralysis, pulselessness.
Intracompartmental pressures > 30 mm Hg require intervention.
Needle pressure gauge (STIC pressure monitor; Stryker, Kalamazoo, MI) if concerned about compartment syndrome.
Underlying fracture assessment.
Secondary reconstruction
Status of soft-tissue coverage (thickness, durability, sensibility, elasticity).
Active and passive range of motion (ROM) of each joint.
Presence of contractures
Discern intrinsic from extrinsic joint contracture.
Assess degree of soft-tissue deficit.
Pertinent imaging or diagnostic studies
Standard radiography (three views of the hand).
Angiography if required for planned free tissue transfer reconstruction.
Blood work: Complete blood cell count (CBC), electrolytes, blood urea nitrogen (BUN), creatinine, international normalized ratio (INR), partial thromboplastin time (PTT), glucose, blood type.
Consider arterial blood gases for associated inhalational injuries or certain chemicals.
Cardiac enzymes, urine myoglobin, creatine kinase, 12-lead electrocardiography for electrical burn.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


