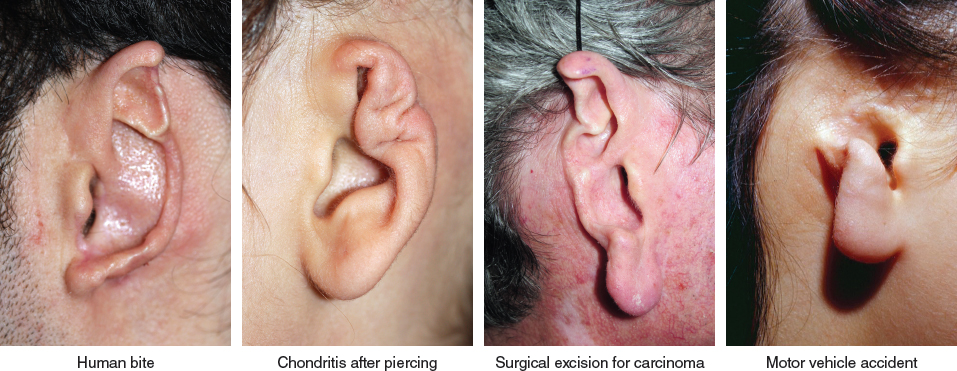
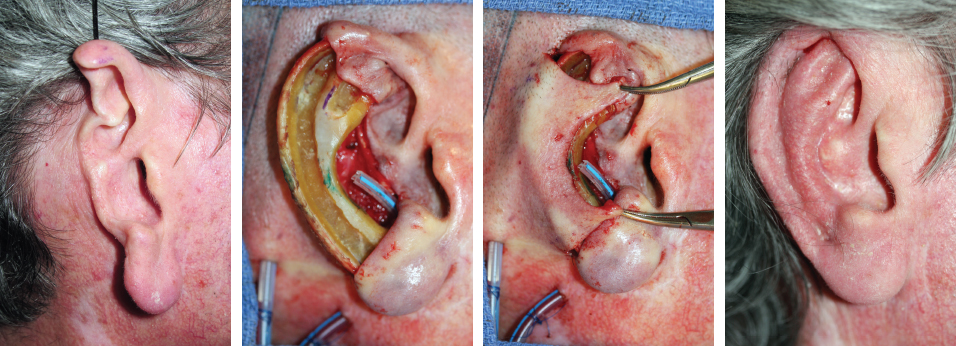
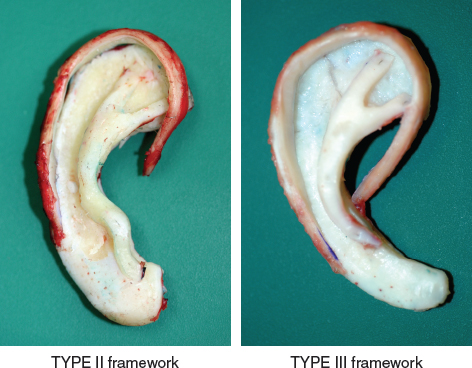
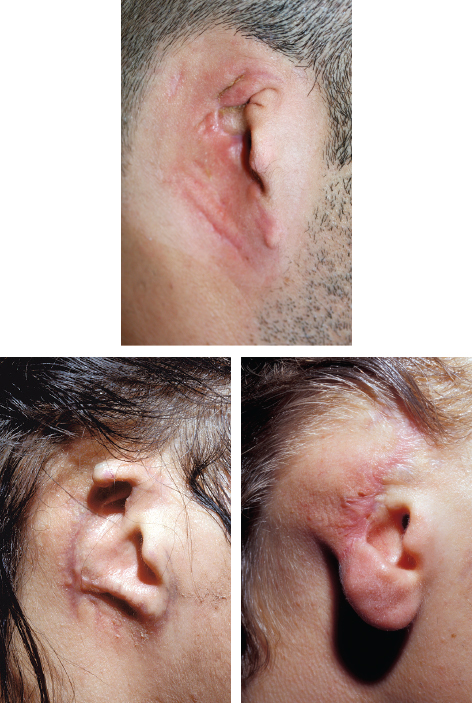
CHAPTER 6 In this chapter we will consider acquired total and subtotal defects of the ear. These cases differ significantly from congenital cases of microtia, because elements of the previously normal ear may still exist, and because the scars must be considered when planning the skin approach. Although the principles of the two-stage autologous technique were developed for microtia, we have also found them to be very useful in the management of acquired defects of the ear. Through our experience, we have developed a separate set of principles specific to acquired defects of the ear. Acquired ear deformities have many causes, including motor vehicle accidents, burns, surgical excision, and animal and human bites. Regardless of the cause, a precise analysis of the local condition of the ear and surrounding skin is necessary. There are three categories of indications for reconstruction: 1. The defect is limited to the ear, with good retroauricular skin. 2. The defect is limited to the ear, with poor retroauricular skin. 3. The defect extends beyond the auricular region. Regardless of the cause of an ear amputation (for example, human bite, chondritis after piercing, surgical excision for carcinoma, and motor vehicle accident, as seen below), the retroauricular skin is often unharmed. This skin is a good texture and color match to the auricular skin and can be used to cover a costal cartilage framework, providing a very good aesthetic result after the first stage. A second stage is required to elevate the reconstructed ear after at least 4 months. In such cases, determining exactly which components of the ear to reconstruct and which skin approach to use is essential. In cases of traumatic amputation, the tragus is usually retained in its normal position. Therefore the choice of framework is between TYPE II and TYPE III. The different types of framework are classified as TYPE I (complete framework, including the tragus and antitragus), TYPE II (without a tragus), and TYPE III (without a tragus and antitragus). Fig. 6-2 If the antitragus is damaged, a TYPE II framework should be used. If it is intact, a TYPE III framework is indicated. In the second case the amputation is subtotal, because the tragus, root of the helix, and anterior part of the helix are undamaged. A TYPE II framework should still be used preserving only the tragus. The third case is a subtotal amputation of the upper and middle thirds. The tragus and antitragus are unharmed and should be retained. The rest of the cartilage should be excised and a TYPE III framework used. Fig. 6-3 The anatomic subunits of the ear need to be respected. The major subunits of the ear are the helix and the antihelix. If the anatomic subunits are not respected, then the junction between the native and reconstructed contours will be visible. When analyzing the defect, deformed contours need to be considered as defects to be removed and reconstructed. Fig. 6-4 This bilateral case shows this principle perfectly. Both sides were reconstructed in one stage. Cartilage was harvested only on the right side of the thorax. On the right side the antihelix was completely deformed. On the left side the antihelix was present but had a deformity of the anterior and posterior roots. A partial reconstruction of the helix and scapha on the left side and a subtotal reconstruction on the right side were performed. The appearance of the antihelix on the right is clearly superior, because the entire subunit, which was deformed, was replaced. The same framework should have been used on the left side, thus harvesting cartilage on both sides of the thorax. Acquired auricular defects almost always retain the tragus, which is the landmark around which the ear can be reconstructed. The depth of the concha determines the normal, three-dimensional contour of the ear; therefore the posterior wall of the concha should always be analyzed for damage. Fig. 6-5 This cannot be considered as simply a partial reconstruction, because the posterior wall of the concha is missing. Although the two roots of the antihelix were preserved, the entire antihelix needed to be reproduced as a subunit. The missing contours, including the antihelix, were carved in one segment of rib cartilage before adding the helix. The final result shows the creation of depth on the conchal bowl, an important feature of a natural result. When operating on adults (as in this case), sufficiently thick cartilage may be present; thus reconstruction of the antihelix and posterior wall of the concha in a single carved piece may be possible. It is only necessary to add the helical portion and secure it with wire. Two types of skin approach are used in acquired ear amputations when good retroauricular skin is available: a type 2 transfixion incision or a type 3b skin incision (see Chapter 1, Principles of the Two-Stage Autologous Ear Reconstruction). Type 2 is a transfixion incision allowing adherence of the portion of the ear comprising anterior and posterior skin surfaces. Part of the framework will be inserted between these two skin layers, and the rest of the framework will be covered by only a single layer and will need secondary elevation. When only the upper portion of the ear has been amputated, a low type 2 skin approach is used, consisting of adhesion of the lobule. This 22-year-old patient had an ear amputation caused by a horse bite. The amputated part of the ear was recovered and brought to the emergency department with the patient immediately after the injury. The surgical team treating the patient removed the skin of the amputated piece and reimplanted the fibrocartilage under the local retroauricular skin. This should never be done, because the elastic fibrocartilage of the ear cannot resist the forces of scar contracture, and the contours will be lost. The deformed fibrocartilage was removed and reconstructed with a TYPE III framework, leaving only the tragus and antitragus, which were unharmed. Several months later the upper part of the ear was elevated to re-create the sulcus (type B). When the lower portion of the ear has been amputated, then a type 2 incision can be used in the reverse fashion, which means that the upper part of the framework will be inserted between the two skin layers of the upper part of the ear. (We call this a high-adhesion high type 2.) Fig. 6-7 This case (see Fig. 6-5) shows a subtotal amputation of the ear caused by a dog bite. The upper part of the ear was preserved. However, the posterior wall of the concha, antihelix, and lobule were missing. NOTE: We do not recommend preserving the upper curvature of the helix unless the whole curvature is undamaged. Attempts to attach normal fibrocartilage to costal cartilage along the curvature frequently lead to a notch in the normal curve of the helix. It is better to join fibrocartilage to costal cartilage in the straight portion of the helix. When only the middle portion of the ear has been amputated, it is possible to use both the upper and lower skin to cover the anterior and posterior surface of part of the framework. A double backcut is then performed, allowing the retroauricular skin to cover the middle portion of the framework.
Acquired Posttraumatic Defects
DEFECT LIMITED TO THE EAR, WITH GOOD RETROAURICULAR SKIN
Analysis of the Missing Contours
Deformed Contours
Posterior Wall of the Concha

Choosing the Best Skin Approach
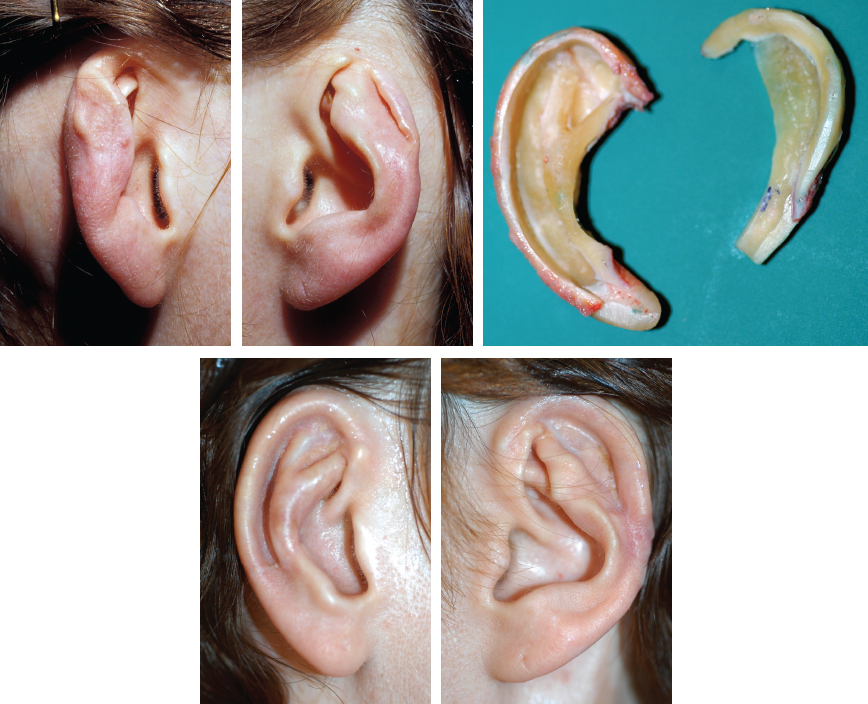
Type 2 Skin Approach in Trauma
Low Type 2
High Type 2

Double Type 2
Plastic Surgery Key
Fastest Plastic Surgery & Dermatology Insight Engine