Key Words
acne, rosacea, perioral dermatitis, hidradenitis, benzoyl peroxide, isotretinoin, hormone therapy, comedonal acne, nodulocystic, erythema, hidradenitis suppurativa
Acne
Acne, a disease of the pilosebaceous unit, appears in males and females who live in westernized societies and are near puberty, and in most cases acne becomes less active as adolescence ends. The intensity and duration of activity vary for each individual.
The disease may be minor, with only a few comedones or papules, or it may occur as the highly inflammatory and diffusely scarring acne conglobata. The most severe forms of acne occur more frequently in males, but the disease tends to be more persistent in females, who may have periodic flare-ups before menstrual periods, which continue until menopause.
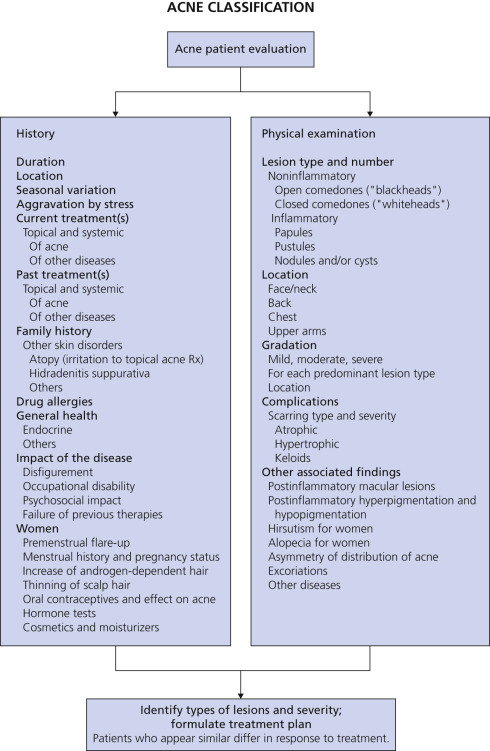
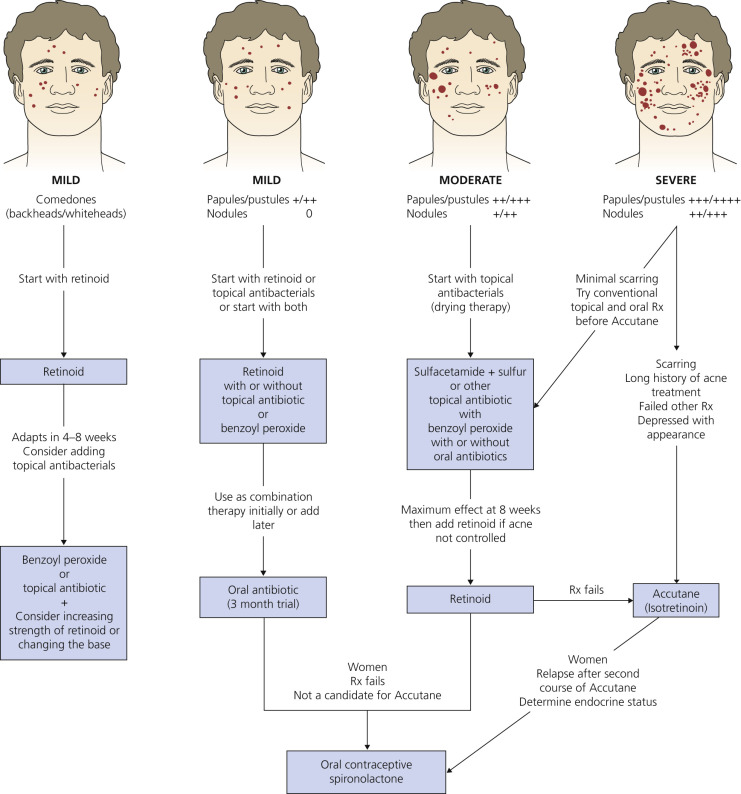
An overview of diagnosis and treatment is presented in Figs. 7.1 to 7.3 and Table 7.1 .

| Agent (Class) | Mechanism of Action | Dosage | Notes |
|---|---|---|---|
| TOPICAL RETINOIDS | |||
| Tretinoin | Comedolysis, induction of orthokeratosis, and inhibition of inflammation | Apply every night; gel: 0.025%, 0.01%; cream: 0.025%, 0.05%, 0.1%; microsponge gel: 0.04%, 0.1% | First-line treatment for all acne. Retinoids as a class are known to cause local skin irritation. Acne exacerbation may occur in early weeks of treatment. Pregnancy category C. |
| Adapalene | Comedolysis, induction of orthokeratosis, and inhibition of inflammation | Apply every night; gel: 0.1% or 0.3%; cream: 0.1% | Alternative first-line treatment for all acne. Retinoids as a class are known to cause local skin irritation. Acne exacerbation may occur in early weeks of treatment. Pregnancy category C. |
| Tazarotene | Comedolysis, induction of orthokeratosis, and inhibition of inflammation | Apply every night; gel: 0.05, 0.1%; cream: 0.05, 0.1% | Second-line treatment for all types of acne because of greater expense, irritation, and lab animal teratogenicity compared with tretinoin and adapalene. Retinoids as a class are known to cause local skin irritation. Acne exacerbation may occur in early weeks of treatment. Pregnancy category X. |
| Salicylic acid (has retinoid properties) | Keratolysis, mild comedolysis | Apply daily to bid; OTC cleanser: 2%; solutions: 0.5%–2% | Nonprescription products useful for mild comedonal acne, adult acne, and keratosis pilaris, mainly in patients with retinoid-intolerant skin. May cause mild local skin irritation. Not recommended for use during pregnancy. |
| TOPICAL ANTIBACTERIALS, ANTIBIOTICS, AND ANTIINFLAMMATORY DRUGS | |||
| Benzoyl peroxide | Potent bactericidal against P. acnes, keratolysis, and comedolysis | Potent bactericidal against P. acnes, keratolysis, and comedolysis: 2.5%, 4%, 5%, 8%, 10% and others; lotions, gels, washes | First-line topical therapy for all acne; reduces comedones and inflammatory lesions, no known resistant bacteria. May cause local skin irritation (5%); contact sensitization (1%–2.5%); bleaching of skin, hair, fabrics, and carpeting; tumor promotion in lab animals. Use lower concentrations (2.5%–4%) for sensitive skin. Pregnancy category C. |
| Clindamycin phosphate | Antibacterial against P. acnes, indirect suppression of inflammation | Apply daily to bid; solution: 1%; pledgets: 1%; gel: 1%; lotion: 1% | Short- to intermediate-term therapy for mild to moderate inflammatory acne. May cause local skin irritation, promotion of antibiotic-resistant bacteria; pseudomembranous enterocolitis has been reported rarely. Pregnancy category B. |
| Erythromycin | Antibacterial against P. acnes, indirect suppression of inflammation | Apply daily to bid; solution: 2%; pledgets: 2%; gel: 2% | Short- to intermediate-term therapy for mild to moderate inflammatory acne. May cause local skin irritation, promotion of antibiotic-resistant bacteria. Pregnancy category B. |
| Dapsone | Antibacterial against P. acnes, indirect suppression of inflammation | Apply daily to bid; gel: 5% Aczone | Short- to intermediate-term therapy for mild to moderate inflammatory acne. May cause local skin irritation. Pregnancy category C. |
| Sulfur/sulfacetamide sodium | Antibacterial against P. acnes, indirect suppression of inflammation; sulfur is a mild keratolytic agent | Apply daily to bid; various OTC and prescription lotions and cleansers: 2%–10% | Adjunctive therapy for mild to moderate teenage and adult acne. May cause local skin irritation and contact reactions in sulfonamide-sensitive patients; has unpleasant odor. Pregnancy category C. |
| Azelaic acid (topical antibiotic, mild anticomedonal drug) | Modest antibacterial activity against P. acnes, modulates keratin formation | Apply bid; cream: 20%; gel: 15% | Adjunctive therapy for mild to moderate acne, especially when hyperpigmentation is present, because of ability to cause hypopigmentation as a side effect. May cause local skin irritation, mainly burning and stinging. Pregnancy category B. |
| COMBINATION TOPICAL ANTIBACTERIALS | |||
| Clindamycin/benzoyl peroxide | Potent bactericidal effect against P. acnes, mild keratolytic agent | Apply daily to bid; gel with clindamycin: 1%; benzoyl peroxide: 5% | More effective than individual components alone; benzoyl peroxide prevents bacterial resistance to clindamycin. See side effects of individual agents above. Pregnancy category C. |
| Erythromycin/benzoyl peroxide | Potent bactericidal effect against P. acnes, mild keratolytic agent | Apply daily to bid; gel with erythromycin: 3%; benzoyl peroxide: 5% | Topical antibacterial and keratolytic combination for all acne; more effective than individual components alone, and benzoyl peroxide prevents bacterial resistance to erythromycin. See side effects of individual agents above. Pregnancy category C. |
| ORAL ANTIBIOTIC DRUGS | |||
| Doxycycline | Antibacterial against P. acnes, indirect suppression of inflammation | 50, 75, 100, or 150 mg PO bid; 75–100 mg PO daily | First line: Modestly priced. May cause dose-related phototoxicity (requires sun protection), vaginal yeast infection, dyspepsia. May be taken with food. Pregnancy category D. Not for acne treatment in children younger than age 12. |
| Minocycline | Antibacterial against P. acnes, indirect suppression of inflammation | 50, 75, or 100 mg PO bid; or extended- release form 55, 65, 80, 105, 115 mg daily | First line: Predictably effective. Higher cost. May cause dizziness, vertigo, discolored teeth, blue-gray skin staining, rare hepatotoxicity and lupus-like syndrome. May be taken with food. Extended-release form is most expensive. Pregnancy category D. Not for acne treatment in children younger than age 12. |
| Ampicillin or amoxicillin | Antibacterial against P. acnes, indirect suppression of inflammation | 500 mg PO bid | Second-line therapy for moderate inflammatory acne. Pregnancy category B. |
| Sulfamethoxazole/trimethoprim | Antibacterial against P. acnes, indirect suppression of inflammation | 1 DS tablet bid | Second-line therapy for severe inflammatory acne. May cause gastric distress, skin rashes, rare Stevens–Johnson syndrome. Useful when isotretinoin is contraindicated. Pregnancy category C. Pediatric use approved after age 2 months. |
| Azithromycin | Antibacterial against P. acnes, indirect suppression of inflammation | 500 mg PO on day 1; 250 mg/day PO on days 2–5; several other schedules are reported in the literature | Second-line therapy for moderate to severe inflammatory acne because of higher cost. May cause gastric upset or diarrhea, rare cholestatic jaundice, and angioedema. Useful in pediatric age group. Pregnancy category B. |
| Tetracycline | Antibacterial against P. acnes, indirect suppression of inflammation | 250 mg PO four times/day, 500 mg PO bid | Availability is erratic. Not widely prescribed. May cause phototoxicity, vaginal yeast infection, dyspepsia, rare liver toxicity, staining of teeth in fetuses and children, reduced efficacy of oral contraceptives. Requires empty stomach; cannot be taken with dairy products. Pregnancy category D. Not for acne treatment in children younger than age 12. |
| Erythromycin | Antibacterial against P. acnes, indirect suppression of inflammation | 1–1.2 g/day PO in divided doses | Erythromycin-resistant P. acnes is a problem. Often causes gastric upset or diarrhea. Useful in pediatric age group. Pregnancy category B. |
| ORAL CONTRACEPTIVE DRUGS AND HORMONAL THERAPY | |||
| Norethindrone acetate/ethinyl estradiol (oral contraceptive) Estrostep | Regulation of androgens by preventing cyclical progesterone surge | 1 pill PO daily for 21 days, skip 7 days, then repeat cycle | First-line treatment of moderate to severe acne in women with laboratory evidence of hyperandrogenism. May cause skin rashes, nausea, vomiting, migraine headaches, mood disorders, hypertension, menstrual irregularities, venous thrombosis, jaundice. Not for use in children or women who are pregnant or lactating. |
| Norgestimate/ethinyl estradiol (oral contraceptive) Ortho Tri-Cyclen | Regulation of androgens by preventing cyclical progesterone surge | 1 pill PO daily for 21 days, skip or take null pill for 7 days, repeat cycle | First-line treatment of moderate to severe acne in women with laboratory evidence of hyperandrogenism. May cause skin rashes, nausea, vomiting, migraine headaches, mood disorders, hypertension, menstrual irregularities, venous thrombosis, jaundice. Not for use in children or women who are pregnant or lactating. |
| Spironolactone (oral antiandrogen) | Spironolactone (oral antiandrogen) | 50–100 mg bid PO | Off-label use for moderate to severe acne in women with laboratory evidence of hyperandrogenism. May cause breast tenderness, frequent menses, hypotension, hyperkalemia, feminization of male fetuses. Pregnancy category C. |
| Prednisone (oral corticosteroid) | Antiinflammatory, suppression of adrenal androgen production | High dose: 40 mg PO daily, tapering to zero over 2–4 weeks; low dose: 5 mg PO daily | High dose: useful for temporary control of severe nodular acne, acne conglobata, and acne fulminans. Low dose: useful for longer-term adrenal suppression in rare cases. May cause gastric distress, fluid retention, increased blood glucose level, hypertension, impaired wound healing, mood swings, growth disturbances, cataracts, glaucoma. Pregnancy category C. |
| ORAL RETINOID DRUG | |||
| Isotretinoin (oral retinoid) | Modulation of epidermal proliferation, induction of orthokeratosis, comedolysis, inhibition of inflammation, and inhibition of sebum secretion | 0.5–2 mg/kg/day PO, daily or divided bid, for 20-wk total course | Treatment of choice for severe, recalcitrant, nodular acne; prolonged remissions (1–3 yr) are seen in about 80% of cases. Side effects include dry skin, chapped lips, dry eyes, nosebleeds, hair loss, major birth defects, hyperlipidemias, transient liver enzyme elevations, musculoskeletal pain, hyperostosis, decreased bone mineral density, diminution of night vision, and psychiatric effects (controversial), including mood swings, depression, suicide risk, and aggressive or violent behavior. Pregnancy category X. All prescribers, patients, wholesalers, and dispensing pharmacies must be registered in the FDA-approved iPLEDGE program ( www.ipledgeprogram.com ). |
Psychosocial Effects of Acne.
Acne is too often dismissed as a minor affliction not worthy of treatment. Believing it is a phase of the growing process and that lesions will soon disappear, parents of children with acne postpone seeking medical advice. Permanent scarring of the skin and the psyche can result from such inaction. The disease has implications far beyond the few marks that may appear on the face. Lesions cannot be hidden under clothing; each is prominently displayed and detracts significantly from one’s personal appearance and self-esteem. Taunting and ridicule from peers is demoralizing. Appearing in public creates embarrassment and frustration. Because acne is perceived by adolescents to have important negative personal and social consequences, improvement in these areas accompanies medical treatment. Facial appearance then becomes more acceptable to peers, embarrassment diminishes, and patients feel less socially inhibited.
The Physician–Patient Relationship.
Many acne sufferers expect to be disappointed with the results of treatment. They may be sensitive to actual or supposed lack of acceptance on the part of their physicians. Adolescence is usually characterized by the challenge of parental rules, and this philosophy transfers to the relationship with the physician. Noncompliance can be decreased by carefully explaining the goals and techniques of treatment and leaving the choice of implementation to the adolescent. Parents who offer to make sure the adolescent follows the treatment plan may encourage noncompliance by placing the treatment within the context of existing parent–child struggles. Greater consideration of adolescents’ psychologic situations improves the therapeutic outcome, increases compliance, and leads to a greater confidence in the physician.
Postadolescent Acne in Women.
A low-grade, persistent acne is common in professional women. Closed comedones are the dominant lesions, with a few papulopustules. Premenstrual flare-ups are typical. Many of these patients passed through adolescence without acne. One author postulated that chronic stress leads to enhanced secretion of adrenal androgens, resulting in sebaceous hyperplasia and subsequent induction of comedones. A survey was taken of adult premenopausal women treated for mild to moderate, nonscarring, inflammatory acne who had undergone standard acne treatments without success or who had a clinical presentation suggesting hyperandrogenism (premenstrual exacerbations, irregular menses, coexisting hirsutism, androgenetic alopecia, seborrhea, or acne distribution on the lower face area, mandibular line, or neck).
The mean duration of acne was 20 years. A mean age at the time of the survey of 37 years and a mean age at onset of 16 years were documented. Acne was reported to be persistent in 80% of the women.
Eighty-three percent reported exacerbation with menses, 67% with stress, and 26% by diet. Pregnancy affected acne in 65% of the women, with 41% reporting improvement and 29% reporting worsening with pregnancy.
Postadolescent Acne in Females and Cigarette Smoking.
The most frequent clinical form of postadolescent acne in females seems to be correlated with cigarette smoking. It consists of retention lesions (microcomedones and macrocomedones), with few inflammatory lesions.
Classification
At the present time, there is no universally accepted acne classification/grading system. A useful acne classification/grading framework employs history and clinical patterns to formulate diagnosis and treatment ( Fig. 7.1 ). This pattern-diagnosis system takes into account the total impact of the disease, which is influenced by the disfigurement it causes. Degree of severity is also determined by occupational disability, psychosocial impact, and the failure of response to previous treatment.
Acne Lesions.
Acne lesions are divided into inflammatory and noninflammatory lesions ( Fig. 7.2 ). Noninflammatory lesions consist of open and closed comedones. Inflammatory acne lesions are characterized by the presence of one or more of the following types of lesions: papules, pustules, and nodules (cysts). Papules are less than 5 mm in diameter. Pustules have a visible central core of purulent material. Nodules are greater than 5 mm in diameter. Nodules may become suppurative or hemorrhagic. Suppurative nodular lesions have been referred to as cysts because of their resemblance to inflamed epidermal cysts. Recurring rupture and reepithelialization of cysts leads to epithelial-lined sinus tracts, often accompanied by disfiguring scars.
Inflammatory acne lesions, may be classified as papulopustular and/or nodular. A severity grade based on a lesion count approximation is assigned as mild, moderate, or severe. Other factors in assessing severity include ongoing scarring, persistent purulent and/or serosanguineous drainage from lesions, and the presence of sinus tracts.
Etiology and Pathogenesis
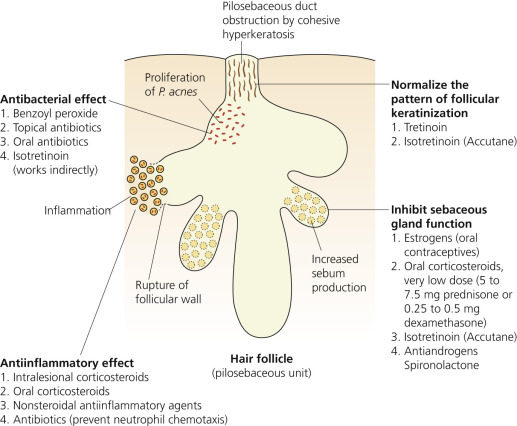
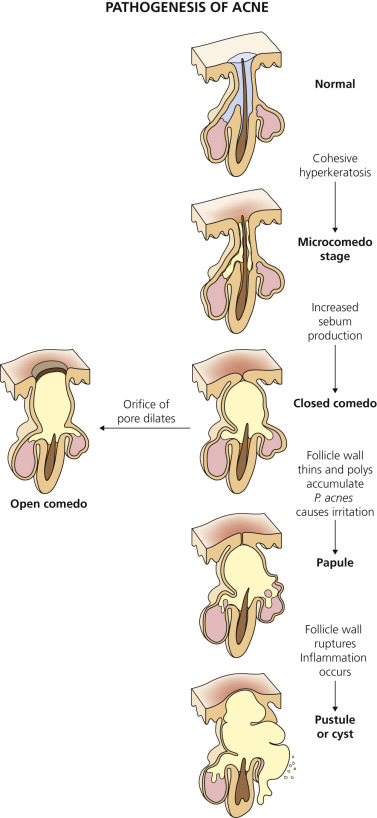
Fig. 7.4 illustrates the mechanism of action of therapeutic agents, and Fig. 7.5 illustrates the evolution of the different acne lesions. Acne is a disease involving the pilosebaceous unit and is most frequent and intense in areas where sebaceous glands are largest and most numerous. Acne begins in predisposed individuals when sebum production increases. Propionibacterium acnes proliferate in sebum, and the follicular epithelial lining becomes altered and forms plugs called comedones.
Sebaceous Glands.
Sebum is the pathogenic factor in acne; it is irritating and comedogenic, especially when P. acnes proliferates and modifies its components. Most patients with acne have a higher than normal sebum level.
Sebaceous glands are located throughout the entire body except the palms, soles, dorsa of the feet, and lower lip. They are largest and most numerous on the face, chest, back, and upper outer arms. Clusters of glands appear as relatively large, visible, white globules on the buccal mucosa (Fordyce spots), the vermilion border of the upper lip ( Fig. 7.6 ), the female areolae (Montgomery tubercles), the labia minora, the prepuce, and around the anus.

Sebaceous glands are large in newborn infants, but regress shortly after birth. They remain relatively small in infancy and most of childhood, but enlarge and become more active in prepuberty. Hormones influence sebaceous gland secretion. Testosterone is converted to dihydrotestosterone (DHT) in the skin and acts directly on the sebaceous gland to increase its size and metabolic rate. Estrogens, through a less well-defined mechanism, decrease sebaceous gland secretion. Sebaceous gland cells produce a complex mixture of oily material. Sebaceous cells mature, die, fragment, and then extrude into the sebaceous duct, where they combine with the desquamating cells of the lower hair follicle and finally arrive at the skin surface as sebum.
Pilosebaceous Duct Obstruction.
The early acne lesion results from blockage in the follicular canal. Increased amounts of keratin result from hormonal changes and sebum modified by the resident bacterial flora P. acnes . The increased number of cornified cells remain adherent to the follicular canal (retention keratosis) directly above the opening of the sebaceous gland duct to form a plug (microcomedo). Factors causing increased sebaceous secretion (puberty, hormonal imbalances) influence the eventual size of the follicular plug. The plug enlarges behind a very small follicular orifice at the skin surface and becomes visible as a closed comedone (firm, white papule). An open comedone (blackhead) occurs if the follicular orifice dilates. Further increase in the size of a blackhead continues to dilate the pore, but usually does not result in inflammation. The small-pore, closed comedone is the precursor of inflammatory acne papules, pustules, and cysts.
Bacterial Colonization and Inflammation.
P. acnes, a Gram-positive anaerobic diphtheroid, is a normal skin resident and the principal component of the microbic flora of the pilosebaceous follicle. P. acnes affects follicular differentiation (microcomedone), increases cutaneous inflammation, and alters lipogenesis and sebum production. This organism activates toll-like receptors, antimicrobial peptides, protease-activated receptors, matrix metalloproteinase and upregulates proinflammatory cytokines (IL-1α, IL-1β, IL-6, IL-8, IL-12. IL-17, TNF-α, granulocyte–macrophage colony-stimulating factor) by keratinocytes, sebaceous cells, and peripheral blood mononuclear cells. P. acnes also promotes microcomedone formation through the insulin-like growth factor (IGF-1) receptor (IGF-1R) pathway. P. acnes generates components that create inflammation, such as lipases, proteases, hyaluronidase, and chemotactic factors. Lipases hydrolyze sebum triglycerides to form free fatty acids, which are comedogenic and primary irritants. Chemotactic factors attract neutrophils to the follicular wall. Neutrophils elaborate hydrolases that weaken the wall. The wall thins, becomes inflamed (red papule), and ruptures, releasing part of the comedone into the dermis. An intense, foreign-body, inflammatory reaction results in the formation of the acne pustule or cyst.
Approach to Acne Therapy
Initial Visit
History.
Many patients are embarrassed to ask for help. Any feeling of apathy or indifference on the part of the physician will be sensed, resulting in a loss of esteem and enthusiasm for the treatment. A careful history should be taken. Inquiring about many details reassures the patient that this is a disease to be taken seriously and managed carefully. Previous treatment should be documented – types of cleansers and lubricants, family history, and history of cyclic menstrual flare-ups. The potential for irritation can be determined by responses to drying therapy with over-the-counter benzoyl peroxide. This experience facilitates the choice of which strength and base of benzoyl peroxide, tretinoin, or other topical agents to prescribe.
Pathogenesis and Course.
Acne is an inherited disease. It is not possible to predict which members of a family will inherit it. The severity of acne in persons developing the disease is not necessarily related to the severity of acne in their parents. Acne does not end at age 19 but can persist into a person’s forties. Many women have their first episode after age 25. Several myths should be discussed. Acne is not caused by dirt. The pigment in blackheads is not dirt and may not be melanin as was once suspected. Excessive washing is unnecessary and interferes with most treatment programs. Gentle manipulation of pustules is tolerated; aggressive pressure and excoriation produces permanent scarring. The erythema and pigmentation that follows resolution of acne lesions in some patients may take many months to fade.
Patients should not have inappropriate expectations. In most cases, acne can be controlled, but not cured. Stress is an important exacerbating factor.
Diet and Family History.
In Western cultures, acne affects up to 95% of adolescents and persists into middle age in 12% of women and 3% of men. Two non-Westernized populations – the Kitavan Islanders of Papua New Guinea and the Aché hunter-gatherers of Paraguay – do not have acne. They eat fruit, fish, game, and tubers but no cereals or refined sugars. This suggests that high-glycemic carbohydrates (bread, bagels, doughnuts, crackers, candy, cake, chips), those that substantially boost blood glucose levels, trigger a series of hormonal changes that cause acne. Elevated blood glucose levels lead to increased insulin production. This affects other hormones that can cause excess oil in the skin. Therefore low-glycemic diets, including fruits and vegetables, might offer a new treatment option for people with acne and some studies support this. Skin biopsies from patients on low-glycemic diets show decrease in size of sebaceous glands, and diminished inflammatory cells and cytokines. Moderate to severe acne is strongly associated with a family history of acne in first-degree relatives. The risk is reduced in people with lower body mass index. The risk is increased with increased milk consumption in those consuming more than 3 portions per week. The association is more marked for skim milk than for whole milk. Online resources are found in Box 7.1 .
Cosmetics and Cleansers.
Moderate use of nongreasy lubricants and water-based cosmetics is usually well tolerated, but a gradual decrease in the use of cosmetics is encouraged as acne improves. Cream-based cleansers should be avoided.
Oral Contraceptives.
If female patients are taking oral contraceptives, a change in estrogen and progestin combinations may be sufficient to improve the prognosis.
Initial Evaluation
Type of Lesions.
An overview of diagnosis and treatment is presented at the beginning of this chapter (see Figs. 7.1 to 7.3 ). The types of lesions present are determined (i.e., comedones, papules, pustules, nodules, or cysts). The degree of severity (mild, moderate, severe) is also determined.
Degree of Skin Sensitivity.
The degree of skin sensitivity can be determined by inquiring about experiences with topical medicines and soaps. Degree of pigmentation and hair color are not the sole determinants of skin sensitivity. Atopic patients with dry skin and a history of eczema generally do not tolerate aggressive drying therapy.
Selection of Therapy.
Therapy appropriate to the type of acne is selected. (For initial orientation, refer to Fig. 7.3 .) If antibiotics are selected for initial therapy, it is best to start with “therapeutic dosages” (see section on Oral Antibiotics, p. 237 ).
Course of Treatment.
A program can be established for most patients after three visits, but some difficult cases require continual supervision. For maximum effect, treatment must be continual and prolonged. Patients who had only a few lesions that quickly cleared may be given a trial period without treatment 6 to 8 weeks after clearing. In an attempt to suppress further activity, those patients who have numerous lesions should continue topical treatment for several months. The patient’s propensity to scar must be ascertained. Patients vary in their tendency to develop scars. Some demonstrate little scarring even after significant inflammation, whereas others develop a scar from nearly every inflammatory papular or pustular lesion. This latter group requires aggressive therapy to prevent further damage. The early use of isotretinoin may be justified in these patients.
Acne Treatment
The following treatment programs are offered only as a guide. Modifications must be made for each individual (see Fig. 7.3 ).
Comedonal Acne
Clinical Presentation.
The earliest type of acne is usually noninflammatory comedones (“blackheads” and “whiteheads”) ( Figs. 7.7 to 7.9 ). It develops in the preteenage or early teenage years and is caused by increased sebum production and abnormal desquamation of epithelial cells. There are no inflammatory lesions because colonization with P. acnes has not yet occurred.



Treatment.
Closed comedone acne (whiteheads) responds slowly. A large mass of sebaceous material is impacted behind a very small follicular orifice. The orifice may enlarge during treatment, making extraction by acne surgery possible. Comedones may remain unchanged for months or evolve into a pustule or cyst.
Topical retinoids (tazarotene, tretinoin, adapalene) are applied at bedtime. The base and strength are selected according to skin sensitivity. Tazarotene may be the most effective and most irritating. Start with a low concentration of the cream or gel (available in 0.05% and 0.1%) and increase the concentration if irritation does not occur. Tretinoin and adapalene are equally effective. Start with tretinoin cream (0.025%, 0.05%, or 0.1%) or gel (0.01% and 0.025%) or with tretinoin gel microsphere (0.04% or 0.1%) or adapalene (gel, cream, solution, pads). Azelaic acid is less potent but is less irritating. It also has antibacterial activity. Medications are used more frequently if tolerated. Add benzoyl peroxide or topical antibiotics or combination medications (e.g., BP–adapalene, BP–clindamycin, clindamycin–tretinoin) later to discourage P. acne and the formation of inflammatory lesions. The response to treatment is slow and discouraging. Several months of treatment are required. Large open comedones (blackheads) are expressed; many are difficult to remove. Several weeks of treatment facilitate easier extraction. Topical therapy may need to be continued for extended periods.
Mild Inflammatory Acne
Clinical Presentation.
Mild pustular and papular inflammatory acne is defined as fewer than 20 pustules. Inflammatory lesions occur in comedones after proliferation of P. acnes . Papules or pustules with a minimum of comedones may develop after comedonal acne ( Figs. 7.10 and 7.11 ).


Treatment.
Benzoyl peroxide, a topical antibiotic, or combination medicine (e.g., BP–clindamycin, BP–hydrocortisone) and a retinoid are initially applied on alternate evenings. The lowest concentrations are initially used. After the initial adjustment period, the retinoid is used each night and benzoyl peroxide or antibiotic is used each morning. The strength of the medications is increased if tolerated. Oral antibiotics are introduced if the number of pustules does not decrease. Topical therapy may require continuation for extended periods. Avoid using topical and oral antibiotics as monotherapy, because monotherapy increases risk of antibiotic resistance.
Moderate to Severe Inflammatory Acne
Clinical Presentation.
Patients who have moderate to severe acne (more than 20 pustules) are temporarily disfigured ( Figs. 7.12 to 7.16 ).





Their disease may have been gradually worsening or may be virulent at the onset. The explosive onset of pustules can sometimes be precipitated by stress. There may be few to negligible visible comedones. Affected areas should not be irritated during the initial stages of therapy.
Treatment.
Many dermatologists will begin with a topical retinoid and combine it with a topical antibiotic. Others will treat with twice-daily application of a topical antibiotic, benzoyl peroxide, or combination medicine (e.g., BP–clindamycin) or the combination of benzoyl peroxide and sulfacetamide/sulfur. This drying agent program can be very effective. Patients using drying agents should adjust the frequency of application to induce a mild, continuous peel. Response to treatment may occur in 2 to 4 weeks. Oral antibiotics (doxycycline or minocycline) are used for patients with more than 10 pustules. Treatment should be continued until no new lesions develop (2 to 4 months) and then should be slowly tapered. If there are any signs of irritation, the frequency and strength of topical medicines should be decreased. Irritation, particularly around the mandibular areas and neck, worsens pustular acne.
A retinoid can be introduced if the number of pustules and the degree of inflammation have decreased. Start minocycline at full dosage if there is no response to doxycycline after 3 months. Pustules are gently incised and expressed. Injecting each pustule with a very small amount of triamcinolone acetonide (2.5 to 5.0 mg/mL) can give immediate and very gratifying results.
Those who have responded well may begin to taper and eventually discontinue oral antibiotics.
Some patients respond very well to lower dosages of oral antibiotics (e.g., doxycycline 20 to 50 mg/day). Those patients may be safely maintained on low-dose oral antibiotics for extended periods. Patients who do not respond to conventional therapy may have lesions that are colonized by Gram-negative organisms. Cultures of pustules and cysts are obtained and an appropriate antibiotic such as ampicillin is started. The response may be dramatic.
Severe: Nodulocystic Acne
Clinical Presentation.
Nodulocystic acne includes pyoderma faciale (inflamed cysts localized on the face in females; Fig. 7.17 ), localized cystic acne (few cysts on face, chest, or back), diffuse cystic acne (wide areas of cysts on face, chest, and back; Figs. 7.18 to 7.28 ), and acne conglobata (highly inflammatory, with cysts that communicate under the skin, abscesses, and burrowing sinus tracts; Figs. 7.29 and 7.30 ).














Cystic Acne
Cystic acne is a serious and sometimes devastating disease that requires aggressive treatment. The face, chest, back, and upper arms may be permanently mutilated by numerous atrophic or hypertrophic scars. Patients sometimes delay seeking help, hoping that improvement will occur spontaneously; consequently, the disease may be quite advanced when first viewed by the physician.
Patients are often embarrassed by and preoccupied with their disease. They may experience anxiety, depression, insecurity, psychic suffering, and social isolation. The physical appearance may be so unattractive that teenagers refuse to attend school and adults fear going to work. Patients report difficulty securing employment when afflicted and problems being accepted in the working environment. Patients with a few inflamed cysts can be treated by implementing a program similar to that outlined for moderate to severe inflammatory acne. Oral antibiotics, conventional topical therapy, and periodic intralesional triamcinolone acetonide injections may keep this problem under adequate control.
Extensive cystic acne requires a different approach. There are three less common variants of cystic acne – pyoderma faciale, acne fulminans, and acne conglobata.
Pyoderma Faciale.
Pyoderma faciale is a distinctive variant of cystic acne that remains confined to the face (see Fig. 7.17 ). It is a disease of adult women ranging in age from the teens to the forties. They experience the rapid onset of large, sore, erythematous-to-purple cysts, predominantly on the central portion of the cheeks. Erythema may be intense. Purulent drainage from cysts occurs spontaneously or with minor trauma. Comedones are absent, and scarring occurs in most cases. A traumatic emotional experience has been associated with some cases. Many patients do not have a history of acne.
Cultures help to differentiate this condition from Gram-negative acne. Highly inflamed lesions can be managed by starting isotretinoin and oral corticosteroids. A study reported effective management with the following: Treatment was begun with prednisolone (1.0 mg/kg daily for 1 to 2 weeks). Isotretinoin was then added (0.2 to 0.5 mg/kg/day [rarely, 1.0 mg/kg in resistant cases]), with a slow tapering of the corticosteroid over the following 2 to 3 weeks. Isotretinoin was continued until all inflammatory lesions resolved. This required 3 to 4 months. None of the patients had a recurrence. This group of patients were “flusher and blushers,” and it was suggested that pyoderma faciale is a type of rosacea. The investigators proposed the term rosacea fulminans.
Acne Fulminans
Acne fulminans is a rare ulcerative form of acne of unknown etiology with an acute onset and systemic symptoms. Tables 7.2 and 7.3 and Fig. 7.31 ![]() summarize the most current classification system, diagnosis and treatment approach to a patient with acne fulminans. It most commonly affects adolescent white boys between the ages of 13 and 22. Many patients have had acne vulgaris for an average of 2 years. A genetic predisposition is suspected, since it has been seen in twins and siblings with similar HLA types. Increased testosterone and anabolic steroid use are risk factors. An ulcerative, necrotic acne with systemic symptoms develops rapidly. There are arthralgias or severe muscle pain, or both, that accompany the acne flare. Painful bone lesions occur in approximately 40% of patients. Weight loss, fever, leukocytosis, and elevated erythrocyte sedimentation rate (ESR) are common findings.
summarize the most current classification system, diagnosis and treatment approach to a patient with acne fulminans. It most commonly affects adolescent white boys between the ages of 13 and 22. Many patients have had acne vulgaris for an average of 2 years. A genetic predisposition is suspected, since it has been seen in twins and siblings with similar HLA types. Increased testosterone and anabolic steroid use are risk factors. An ulcerative, necrotic acne with systemic symptoms develops rapidly. There are arthralgias or severe muscle pain, or both, that accompany the acne flare. Painful bone lesions occur in approximately 40% of patients. Weight loss, fever, leukocytosis, and elevated erythrocyte sedimentation rate (ESR) are common findings.
| Term | Abbreviation | Definition |
|---|---|---|
| Acne fulminans with systemic symptoms | AF-SS | Abrupt, dramatic flare of inflammatory acne, with erosions +/− crusts, ulcers, hemorrhagic nodules/plaques, as well as systemic findings (fever, malaise, bone pain, arthralgias, erythema nodosum, and leukocytosis) Laboratory abnormalities might include anemia, leukocytosis, elevated erythrocyte sedimentation rate, and C-reactive protein X-ray findings: Osteolytic bony lesions; usual sites include sternum, clavicles, sacroiliac joints, hips |
| Acne fulminans without systemic symptoms | AF-WOSS | Abrupt, dramatic flare of inflammatory acne, with erosions +/− crusts, ulcers, and hemorrhagic nodules/plaques without systemic findings |
| Isotretinoin-induced acne fulminans with systemic symptoms | IIAF-SS | Drug-induced form of acne fulminans with systemic symptoms (rarely testosterone and anabolic steroids can induce this reaction; this entity is much less common than IIAF-WOSS) |
| Isotretinoin-induced acne fulminans without systemic symptoms | IIAF-WOSS | Drug-induced form of acne fulminans without systemic symptoms (other drugs including testosterone and anabolic steroids can induce IIAF-WOSS; this entity is the most common form of AF) |
| Physical Examination | Complete Physical Examination Including Temperature |
|---|---|
| Laboratory studies |
|
| Imaging | Radiograph (only if patient has symptoms concerning for bone or joint involvement) |
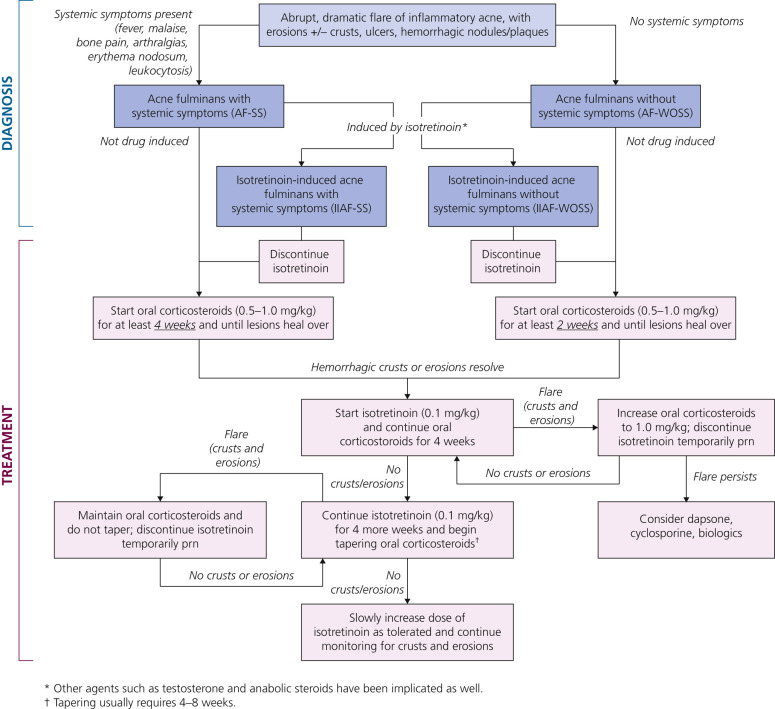
Antibiotic therapy is not effective. Oral corticosteroids (e.g., prednisolone or prednisone 0.5 to 1.0 mg/kg) are the primary therapy. They quickly control the skin lesions and systemic symptoms. Isotretinoin (0.5 mg/kg) is started simultaneously and, as in the therapy of severe cystic acne, is continued for 5 months. Start with a low dosage of isotretinoin. High dosages may precipitate inflamed lesions with granulation tissue. The duration of steroid therapy is often at least 2 months. The bone lesions have a good prognosis; chronic sequelae are rare.
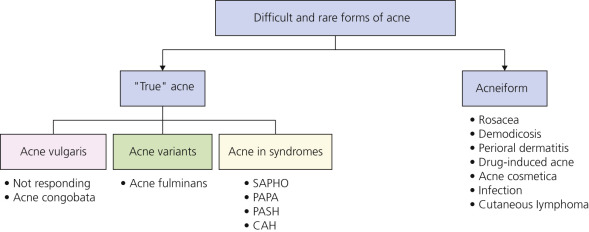
Table 7.4 and Fig. 7.32 summarize distinguishing characteristics of rare and difficult to diagnosis forms of acne vulgaris.
| Condition | Patient History | Clinical Presentation | Laboratory Evaluations | Skin Biopsy | Imaging |
|---|---|---|---|---|---|
| Acne fulminans | Adolescent boys Precipitated by oral isotretinoin intake, possible | Sudden onset of hemorrhagic ulcerative acne mainly on the trunk Fever, myalgias, arthralgias | Anemia, leukocytosis | Hemorrhagic epidermal necrosis Granulocytes in dermis | Focal lytic bone lesions or sacroiliitis may be present |
| SAPHO syndrome | Rarely, children and young adults | Any of the 3 criteria: (1) chronic recurrent multifocal osteomyelitis with or without skin clinical manifestations; (2) acute or chronic sterile arthritis with either pustular psoriasis or palmoplantar pustulosis or severe acne; (3) sterile osteitis in the presence of one of the skin manifestations | RF: Negative | NA | Bone scintigraphy: Sternoclavicular involvement. Magnetic resonance imaging of the dorsal spine: Hyperfixation and enhancement of vertebral plates (spondylodiscitis), sternoclavicular synovitis CT of the dorsal spine: Sternal hyperostosis, erosion of the vertebral plates |
| PAPA syndrome | Hereditary (mutations in CD2 BP1 ) with variable penetration | Pyogenic sterile arthritis, pyoderma gangrenosum, acne conglobata | Seronegative arthritis | NA | Pauciarticular, usually nonaxial arthritis |
Acne Conglobata
Acne conglobata is a chronic, highly inflammatory form of cystic acne in which involved areas contain a mixture of double comedones (two blackheads that communicate under the skin), papules, pustules, communicating cysts, abscesses, and draining sinus tracts (see Figs. 7.25 and 7.30 ). The disease may linger for years, ending with deep atrophic or keloidal scarring. Acne conglobata is part of the rare follicular occlusion triad syndrome of acne conglobata, hidradenitis suppurativa (HS), and dissecting cellulitis of the scalp (see Fig. 7.29 and Fig. 7.33 ). Musculoskeletal symptoms have been reported in some of these patients; 85% were black. There is no fever or weight loss as is seen in acne fulminans.

Treatment of Nodulocystic Acne
The patient is assured that effective treatment is available. Patients should be told that they will be observed closely and, if the disease becomes very active, they will be seen at least weekly until the condition is adequately controlled. A primary therapeutic goal is to avoid scarring by terminating the intense inflammation quickly; prednisone is sometimes required. Cysts with thin roofs are incised and drained. Deeper cysts are injected with triamcinolone acetonide (2.5 to 10 mg/mL).
Patients who show little tendency to scar can be treated as patients with moderate to severe inflammatory acne. Most patients will require the rapid introduction of isotretinoin. Start with low dosages of isotretinoin (0.5 mg/kg or less) to avoid exacerbation of lesions that may have granulation tissue. The simultaneous use of tetracyclines (tetracycline, doxycycline, or minocycline) and isotretinoin is avoided, because a higher incidence of pseudotumor cerebri may occur with this combination. For highly active cases, prednisone (adult dosage is 20 to 30 mg two times a day) is used.
Intralesional triamcinolone acetonide injections and incision and drainage of cysts are important in the early weeks of management. Patients taking isotretinoin are usually not treated with other oral or topical agents.
Treatment of Acne in Pregnancy
There are no clear guidelines for treatment of acne during pregnancy. Most women want to know that a therapy is 100% safe for the baby. Tables 7.5 to 7.9 are guidelines for treatment of acne during pregnancy.
| Category A | Adequate, well-controlled studies in pregnant women have not shown an increased risk of fetal abnormalities. |
| Category B | Animal studies have revealed no evidence of harm to the fetus; however, there are no adequate and well-controlled studies in pregnant women or Animal studies have shown an adverse effect, but adequate and well-controlled studies in pregnant women have failed to demonstrate a risk to the fetus. |
| Category C | Animal studies have shown an adverse effect, and there are no adequate and well-controlled studies in pregnant women or No animal studies have been conducted, and there are no adequate and well-controlled studies in pregnant women. |
| Category D | Adequate well-controlled or observational studies in pregnant women have demonstrated a risk to the fetus. However, the benefits of therapy may outweigh the potential risk. |
| Category X | Adequate well-controlled or observational studies in animals or pregnant women have demonstrated positive evidence of fetal abnormalities. The use of the product is contraindicated in women who are or may become pregnant. |
| Type of Acne | Treatment | FDA Pregnancy Drug Class | Evidence Rating |
|---|---|---|---|
| NONINFLAMMATORY | |||
| Comedonal | Azelaic acid | B | Likely to be beneficial |
| INFLAMMATORY | |||
| Mild to moderate | Azelaic acid + | B | Likely to be beneficial |
| Benzoyl peroxide or | C | Beneficial | |
| Topical erythromycin or | B | Beneficial | |
| Topical clindamycin + | B | Beneficial | |
| Benzoyl peroxide | C | Beneficial | |
| Moderate to severe | Oral erythromycin or | B | Likely to be beneficial |
| Oral cephalexin + | B | * | |
| Benzoyl peroxide with or without | C | Beneficial | |
| Azelaic acid or | B | Likely to be beneficial | |
| Intralesional steroid injections | C | * | |
| Fulminant | Oral erythromycin + | B | Likely to be beneficial |
| Benzoyl peroxide + | C | Beneficial | |
| Azelaic acid + | B | Likely to be beneficial | |
| Oral prednisone (short-term) | C | * | |
* Evidence of a drug’s benefit is not discussed in source article.
| Agent | FDA Category | Mechanism of Action | Available Formulations | Notes |
|---|---|---|---|---|
| Azelaic acid | B | Antimicrobial Comedolytic Antiinflammatory Antityrosinase activity | Cream (20%; approved for acne) Gel (15%; approved for rosacea) | Monotherapy is possible No known bacterial resistance Can improve postinflammatory hyperpigmentation |
| Benzoyl peroxide | C | Antibacterial Comedolytic Antiinflammatory | Wash, bar, pad, gel, mask, foam, lotion, cream (2.5%–10%) | Monotherapy is possible No known bacterial resistance Can cause bleaching |
| Salicylic acid | C | Comedolytic Keratolytic | Lotion, cleanser, gel, cream, foam, soap, toner, pads (0.5%–6%) | Generally well-tolerated by patients Less effective than azelaic acid or benzoyl peroxide |
| Erythromycin | B | Antibacterial | Gel, solution, pad, ointment (2%) Erythromycin/benzoyl peroxide gel (3%/5%) | Should not to be used as monotherapy Bacterial resistance is diminished by combining with benzoyl peroxide |
| Clindamycin | B | Antibacterial | Gel, lotion, solution, foam, swab (1%) Clindamycin/benzoyl peroxide gel (1%/5%, 1.2%/2.5%) | Should not to be used as monotherapy Use with caution in patients with a history of gastrointestinal disease Bacterial resistance is diminished by combining with benzoyl peroxide |
| Tazarotene | X | Comedolytic Antiinflammatory | Cream, gel, foam (0.05%/0.1%) | Contraindicated in pregnancy |
| Tretinoin | C | Comedolytic Antiinflammatory | Gel (0.01%/0.025%/0.05%), microsphere gel (0.04%/0.08%/0.1%), cream (0.02%–0.1%), topical solution (0.05%) | Not recommended in pregnancy |
| Adapalene | C | Comedolytic Antiinflammatory | Lotion, cream (0.1%) Gel (0.1%/0.3%) Adapalene/benzoyl peroxide gel (0.1%/2.5%) | Not recommended in pregnancy |
| Dapsone | C | Antiinflammatory Antimicrobial | Gel (5%) | Low risk of maternal anemia, neonatal hyperbilirubinemia, and hemolytic anemia in patients with G6PD deficiency (for topical dapsone) |
| Agent | FDA Pregnancy Category | Dosage | Notes |
|---|---|---|---|
| Erythromycin | B | 250–500 mg, 2–4 times/day | Long-term use in pregnancy has not been studied Bacterial resistance is diminished by combining with topical benzoyl peroxide Hepatotoxicity is associated with erythromycin estolate; not recommended for pregnancy |
| Azithromycin | B | Dosing routine may vary, e.g., 250 mg, 3 times/week | Off-label indication More flexible dosing regimen for less compliant patients |
| Cephalexin | B | 500 mg twice daily | Concern for Staphylococcus resistance |
| Amoxicillin | B | 250–500 mg twice daily | Use in early pregnancy may increase risk of oral clefts |
| Trimethoprim/sulfamethoxazole | C | 160/800 mg twice per day | Exposure during the first trimester is associated with miscarriage |
| Tetracycline | D | 250–500 mg twice daily | Toxic effects on fetal teeth and bone Avoid in pregnancy |
| Minocycline or doxycycline | D | 50–100 mg once or twice per day | Toxic effects on fetal teeth and bone Avoid in pregnancy |
| Clinical Recommendation | Evidence Rating * | References |
|---|---|---|
| Topical azelaic acid (15% or 20%) and benzoyl peroxide (2.5%–5%) are effective baseline agents. | B | |
| Topical erythromycin in combination with benzoyl peroxide (5% maximum) can be used as alternative treatment for inflammatory acne. | C | |
| Topical clindamycin in combination with benzoyl peroxide can be used as alternative treatment for inflammatory acne. | C | |
| Topical dapsone is a newer anti-acne agent with less available safety data and should be used with caution in pregnant patients. | C | |
| Topical and oral antibiotics (e.g., erythromycin) should be used in combination with benzoyl peroxide to reduce the risk of bacterial resistance. | C | |
| Oral cephalexin can be used in moderate to severe inflammatory acne. | C | |
| Intralesional steroid injections can be used to treat moderate to severe inflammatory acne. | C | |
| Oral glucocorticoids can be used short term to treat fulminant acne after the first trimester. | C |
* B, inconsistent or limited-quality patient-oriented evidence; C, consensus, disease-oriented evidence, usual practice, expert opinion, or case series. For information about the Strength of Recommendation Taxonomy evidence rating system, go to www.aafp.org/afp/2004/0201/p548.html
Therapeutic Agents for Treatment of Acne
There are four pathogenetic factors responsible for the development of acne. These are hyperkeratinization (plugging) of the pilosebaceous follicles, increased testosterone levels (producing hyperseborrhea), bacterial colonization with P. acnes, and inflammation. Topical agents influence at least one of these factors. More than 50% of patients present with comedones and papulopustular acne. These patients are initially treated with topical medications. Combination regimens that include an antibiotic and a retinoid to reduce follicular plugging are the mainstay of topical treatment. Pustular acne may respond quickly to drying therapy with a combination of benzoyl peroxide and sulfacetamide-sulfur lotion. Systemic therapy with antibiotics or isotretinoin is used when scarring occurs or for cystic acne.
Topical and oral agents act at various stages (see Fig. 7.5 ) in the evolution of an acne lesion and may be used alone or in combination to enhance efficacy. Topical agents should be applied to the entire affected area to treat existing lesions and to prevent the development of new ones. Potent topical steroid creams produce no short-term improvement in patients with moderate acne.
Retinoids
Retinoids reverse the abnormal pattern of keratinization seen in acne vulgaris. Agents that act in a comedolytic and anticomedogenic manner to reduce follicular plugging are the retinoids tretinoin, adapalene, and tazarotene, and isotretinoin. Adapalene has antiinflammatory activity. Retinoids may cause an increase in facial dryness and erythema.
Mechanism of Action.
Retinoids initiate increased cell turnover in both normal follicles and comedones and reduce the cohesion between keratinized cells. They act specifically on microcomedones (the precursor lesion of all forms of acne), causing fragmentation and expulsion of the microplug, expulsion of comedones, and conversion of closed comedones to open comedones. New comedone formation is prevented by continued use. Inflammation may occur during this process, temporarily worsening the acne. Continual topical application leads to thinning of the stratum corneum, making the skin more susceptible to sunburn, sun damage, and irritation from wind, cold, or dryness. Irritants such as astringents, alcohol, and acne soaps will not be tolerated as they were previously. The incidence of contact allergy is very low . Because of the direct action of retinoids on the microcomedone, many clinicians believe retinoids are appropriate for all forms of acne.
Combination Therapy – Synergism.
Retinoids enhance the penetration of other topical agents such as topical antibiotics and benzoyl peroxide. The enhanced penetration results in a synergistic effect with greater overall drug efficacy and a faster response to treatment.
Adapalene–Benzoyl Peroxide Combination.
The fixed-dose adapalene 0.1%–benzoyl peroxide 2.5% and adapalene 0.3%–benzoyl peroxide combination gel are efficacious and safe acne treatments. The relative benefit of adapalene–benzoyl peroxide increases with higher lesion counts at baseline.
Clindamycin–Tretinoin Combination (CT).
CT gel is more effective than clindamycin or tretinoin monotherapy. The CT gel produced significantly less burning/stinging and pruritus than the adapalene–benzoyl peroxide combination.
Application Techniques.
The skin should be washed gently with a mild soap (e.g., Purpose, Basis) no more than two to three times each day, using the hands rather than a washcloth. Special acne or abrasive soaps should be avoided. To minimize possible irritation, the skin should be allowed to dry completely by waiting 20 to 30 minutes before application of retinoids. The retinoid is applied in a thin layer once daily. Medication is applied to the entire area, not just to individual lesions. A pea-sized amount is enough for a full facial application. Patients with sensitive skin or those living in cold, dry climates may start with an application every other or every third day. The frequency of application can be gradually increased to as often as twice each day if tolerated. The corners of the nose, the mouth, and the eyes should be avoided; these areas are the most sensitive and the most easily irritated. Retinoids are applied to the chin less frequently during the initial stages of therapy; the chin is sensitive and is usually the first area to become red and scaly. Sunscreens should be worn during the summer months if exposure is anticipated.
Response to Treatment.
One to four weeks: During the first few weeks, patients may experience redness, burning, or peeling. Those with excessive irritation should use less frequent applications (i.e., every other or every third day). Most patients adapt to treatment within 4 weeks and return to daily applications. Those tolerating daily applications may be advanced to a higher dosage or to the more potent solution.
Three to six weeks: New papules and pustules may appear because comedones become irritated during the process of being dislodged. Patients unaware of this phenomenon may discontinue treatment. Some patients do not worsen and sometimes begin to improve dramatically by the fifth or sixth week.
After six weeks: Most patients improve by the ninth to twelfth week and exhibit continuous improvement thereafter. Some patients never adapt to retinoids and experience continuous irritation or continue to worsen. An alternate treatment should be selected if adaptation has not occurred by 6 to 8 weeks. Some patients adapt but never improve. Retinoids may be continued for months to prevent appearance of new lesions.
Tretinoin.
Tretinoin is effective for noninflammatory acne consisting of open and closed comedones. It is available in various preparations (see the Formulary).
Tazarotene.
Tazarotene is available as a gel (0.05%, 0.1%), a cream (0.05%, 0.1%), and a foam (0.1%). Tazarotene 0.1% gel (once daily) is more effective than tretinoin 0.025% gel (once daily) in reducing the numbers of papules and open comedones, and achieves a more rapid reduction in pustules in mild to moderate facial acne. Alternate-day tazarotene 0.1% gel is as effective as once-daily adapalene 0.1% gel. The tolerability of tazarotene gel is comparable to that of tretinoin 0.025% gel, tretinoin 0.1% gel microsphere, and adapalene 0.3% gel. Tolerability of tazarotene is better when therapy is initiated with an alternate-day regimen.
A short contact method may be effective. Apply the gel for just a few minutes; then wash it off. Tazarotene may be left in contact for increasing intervals until overnight application is tolerated.
Adapalene.
Adapalene is available as a gel or cream. It has tretinoin-like activity in the terminal differentiation process of the hair follicle. Adapalene has antiinflammatory activity. Adapalene gel 0.1% is as effective as 0.025% tretinoin gel for mild to moderate acne. It is better tolerated than tretinoin gel. It does not cause sun sensitivity. Adapalene gel 0.3% is also available.
Azelaic Acid.
Azelaic acid cream is a naturally occurring compound that has antikeratinizing, antibacterial, and antiinflammatory properties. It is effective for noninflammatory and inflammatory acne. Azelaic acid has strong antibacterial potency without inducing bacterial resistance, similar to benzoyl peroxide. It is an effective monotherapy in mild to moderate forms of acne, with an overall efficacy comparable to that of tretinoin (0.05%), benzoyl peroxide (5%), and topical erythromycin (2%). Its efficacy can be enhanced when it is used in combination with other topical medications such as benzoyl peroxide 4% gel, clindamycin 1% gel, tretinoin 0.025% cream, and erythromycin 3%/benzoyl peroxide 5% gel. Azelaic acid cream may be combined with oral antibiotics for the treatment of moderate to severe acne and may be used for maintenance therapy when antibiotics are stopped. It does not cause sun sensitivity or significant local irritation. It does not induce resistance in P. acnes .
Benzoyl Peroxide
The primary effect of benzoyl peroxide is antibacterial; therefore it is most effective for inflammatory acne consisting of papules, pustules, and cysts, although many patients with comedone acne respond to it. Benzoyl peroxide is less effective than tretinoin at disrupting the microcomedo. Benzoyl peroxide and isotretinoin significantly reduce noninflamed lesions in 4 weeks. In one study, benzoyl peroxide had a more rapid effect on inflamed lesions with significant reductions at 4 weeks, whereas the use of isotretinoin showed a significant improvement at 12 weeks.
Benzoyl peroxide is available over the counter and by prescription. Some examples of benzoyl peroxide preparations are water-based gel (Benzac AC 2.5%, 5%, and 10%), alcohol-based gel (Benzagel 5% and 10%), and acetone-based gel (Persa-Gel 5% and 10%) (see the Formulary). Water-based gels are less irritating, but alcohol-based gels, if tolerated, might be more effective. Benzoyl peroxide is also available in a soap base in strengths from 2.5% to 10%.
Benzoyl Peroxide/Antibiotic Formulations.
The combinations of erythromycin/benzoyl peroxide and clindamycin/benzoyl peroxide are superior for inflammatory and noninflammatory acne versus either ingredient used alone. The clindamycin/benzoyl peroxide combination gel has an advantage over erythromycin/benzoyl peroxide gel because the former does not require refrigeration. The two products have similar efficacy. Benzoyl peroxide–hydrocortisone (5%–0.5%) is available and very effective for inflammatory lesions.
Benzoyl peroxide produces a drying effect that varies from mild desquamation to scaliness, peeling, and cracking. Patients should be reassured that drying does not cause wrinkles. Benzoyl peroxide causes a significant reduction in the concentration of free fatty acids via its antibacterial effect on P. acnes . This activity is presumably caused by the release of free radical oxygen, which is capable of oxidizing bacterial proteins. Benzoyl peroxide seems to reduce the size of the sebaceous gland, but whether sebum secretion is suppressed is still unknown. Patients should be warned that benzoyl peroxide is a bleaching agent that can ruin clothing.
Principles of Treatment.
Benzoyl peroxide should be applied in a thin layer to the entire affected area. Most patients experience mild erythema and scaling during the first few days of treatment, even with the lowest concentrations, but adapt in a week or two. It was previously believed that vigorous peeling was necessary for maximum therapeutic effect; although many patients improved with this technique, others became worse. An adequate therapeutic result can be obtained by starting with daily applications of the 2.5% or 5% gel and gradually increasing or decreasing the frequency of applications and strength until mild dryness and peeling occur.
Allergic Reaction.
Approximately 2% of patients develop allergic contact dermatitis from benzoyl peroxide and must discontinue its use. The sudden appearance of diffuse erythema and vesiculation suggests contact allergy to benzoyl peroxide.
Drying and Peeling Agents
The oldest technique for treating acne is to use agents that induce a continuous mild drying and peeling of the skin. In selected patients, especially those with pustular acne, this technique may provide fast and effective results. Prescription and over-the-counter products used for this purpose contain sulfur, salicylic acid, resorcinol, and benzoyl peroxide. Before the use of tretinoin and antibiotics, this approach secured very acceptable results for many patients.
The goal is to establish a mild continuous peel by varying the frequency of application and the strength of the agent. Treatment is stopped temporarily if dryness becomes severe. The drying and peeling technique can be recommended to patients who are reluctant to visit the physician or to parents inquiring about children who are beginning to develop acne. If improvement is negligible after an 8-week trial, the patient should consider evaluation by a physician. Two effective agents are benzoyl peroxide and sulfacetamide 10%, sulfur 5% lotion. One is used in the morning and the other in the evening or as often as tolerated.
Topical Antibiotics
Topical antibiotics are useful for mild pustular and comedonal acne. They can be prescribed initially or as adjunctive therapy after the patient has adapted to tretinoin or benzoyl peroxide. Clinical trials have demonstrated that application twice a day is as effective as oral tetracycline 250 mg taken twice daily or minocycline 50 mg taken twice daily. Most solutions are alcohol-based and may produce some degree of irritation. Cleocin T lotion does not contain propylene glycol and for some patients may be less irritating. Clindamycin (Cleocin T pads, solution, and lotion) is a commonly used topical antibiotic. Dapsone gel 5% has antibiotic and antiinflammatory properties. Topical antibiotics should not be used as monotherapy because of induction of antibiotic resistance, especially Staphylococcus aureus . They should be combined with a topical retinoid or benzoyl peroxide.
Oral Antibiotics
Antibiotics have been used for approximately four decades for the treatment of papular, pustular, and cystic acne (see Table 7.1 ).
Mechanism of Action and Dosage.
The major effect of antibiotics is believed to ensue from their ability to decrease follicular populations of P. acnes . The role of P. acnes in the pathogenesis of acne is not completely understood. Neutrophil chemotactic factors are secreted during bacterial growth, and these may play an important role in initiating the inflammatory process. Because several antibiotics used to treat acne can inhibit neutrophil chemotaxis in vitro , they are thought to act as an antiinflammatory agent. Subminimal inhibitory concentrations of minocycline were shown to have an antiinflammatory effect by inhibiting the production of neutrophil chemotactic factors in comedonal bacteria. Antibiotic-resistant strains of P. acnes have been discovered.
Antibiotic-Resistant Propionibacteria and Long-Term Therapy.
P. acnes is sensitive to several antibiotics but the prevalence of P. acnes resistant to antibiotics is increasing. Resistance genes are easily transferred among different bacteria. After treatment with both systemic and oral antibiotics, P. acnes develops resistance in more than 50% of cases, and it is estimated that one in four acne patients harbors strains resistant to tetracycline, erythromycin, and clindamycin. Resistance to minocycline is less common. Carriage of resistant strains results in therapeutic failure of some but not all antibiotic regimens. In many patients with acne, continued treatment with antibiotics can be inappropriate or ineffective. It is important to recognize therapeutic failure and alter treatment accordingly. The use of long-term rotational antibiotics is outdated and will only exacerbate antibiotic resistance.
Dosage and Duration.
Better clinical results and a lower rate of relapse after stopping antibiotics are achieved by starting at higher dosages and tapering only after control is achieved. Typical starting dosages are doxycycline 100 mg once daily or twice daily, minocycline 100 mg twice daily, and amoxicillin 500 mg twice daily. Antibiotics are prescribed in divided doses; there is better compliance with twice-a-day dosing. Antibiotics must be taken for weeks to be effective and are used for many weeks or several months to achieve maximum benefit, but their use should be limited to 3 to 4 months. Attempts to control acne with short courses of antibiotics (less than 2 weeks), as is often tried to prevent premenstrual flare-ups of acne, are usually not effective.
Tetracycline Antibiotics.
The prolonged use of tetracycline antibiotics lowered the prevalence of colonization by Staphylococcus aureus and did not increase resistance to the tetracycline antibiotics.
Tetracycline.
Tetracycline is not widely prescribed for acne, due to lack of availability. One major disadvantage is the requirement that tetracycline not be taken with food (particularly dairy products), certain antacids, and iron, all of which interfere with the intestinal absorption of the drug. Failure to adhere to these restrictions accounts for many of the reported therapeutic failures of tetracycline.
Dosing.
Efficacy and compliance are obtained by starting tetracycline administration at 500 mg twice each day and continuing this dosage until a significant decrease in the number of inflamed lesions occurs, usually in 3 to 6 weeks. Thereafter the dosage may be decreased to 250 mg twice each day, or oral therapy may be discontinued in favor of topical antibiotics. Patients who do not respond after 6 weeks of adequate dosages of oral tetracycline should be introduced to an alternative treatment. For unknown reasons a significant number of patients who take tetracycline exactly as directed do not respond to high dosages, whereas others respond very favorably to 250 mg once a day or once every other day and experience flare-ups when attempts are made to discontinue treatment.
Adverse Effects.
The incidence of photosensitivity to tetracycline is low, but it increases when higher dosages are used. All females should be warned about the increased incidence of Candida albicans vaginitis. The package labeling of oral contraceptives warns that reduced efficacy and increased incidence of breakthrough bleeding may occur with tetracycline and other antibiotics. Although this association has not been proven, it is prudent to inform patients of this potential risk. Pseudotumor cerebri, a self-limited disorder in which the regulation of intracranial pressure is impaired, is a rare complication of tetracycline treatment. Increased intracranial pressure causes papilledema and severe headaches. Increased intraocular pressure can lead to progressive visual impairment and eventually blindness.
Doxycycline.
Doxycycline is a safe and effective medication. It is commonly prescribed for acne. Studies of doxycycline (50 and 100 mg) showed no significant difference between its clinical efficacy and that of minocycline in treating acne. Doxycycline is less expensive than minocycline. The incidence of photosensitivity increases with increasing dose levels ( Fig. 7.34 ).










