Achilles Tendon Reconstruction
Hani Sbitany
DEFINITION
Achilles tendon is the most frequently ruptured tendon in the body, with incidence reported as high as 34/100 000, most commonly seen in males in their 30s.1
The male-to-female ratio of this injury is 20:1.
Classically seen when less active males engage in a new sport, without significant previous experience.
ANATOMY
Most common site of rupture is 3 to 6 cm above the os calcis (ie, the calcaneus):
This area is a watershed zone in terms of blood supply.
Achilles tendon is made up of gastrocnemius and soleus muscles, along with the plantaris tendon (FIG 1).
This tendon begins in the midportion of the calf (superficial posterior compartment) and narrows to approximately 4 cm width at its insertion on the calcaneus bone.
Achilles tendon helps to produce plantar flexion of the foot, which is powered through associated muscle innervation by the tibial nerve.
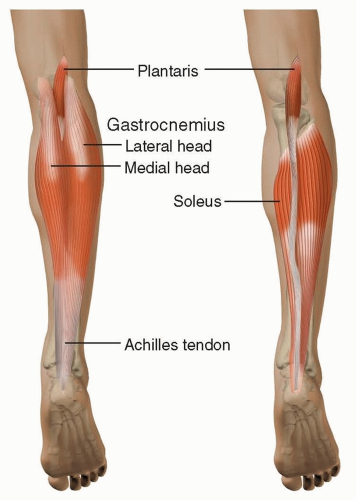 FIG 1 • The Achilles tendon is formed by the convergence of the medial, lateral gastrocnemius, and soleus muscles. |
PATHOGENESIS
With aging, there is an increase in type 3 collagen content on the Achilles tendon and a reduction in type 1 collagen content.2
Increasing age is also accompanied by decreased orderly collagen cross-linking.
All this results in reduced tensile strength of the tendon.
NATURAL HISTORY
In addition to aging, there are numerous other risk factors associated with Achilles tendon rupture:
Hypercholesterolemia
Rheumatoid arthritis
Hypercholesterolemia
Long-term dialysis
Renal transplantation
Chronic steroid use
PATIENT HISTORY AND PHYSICAL FINDINGS
A history of pain and weakening on plantar flexion is usually indicative of Achilles tendon rupture.
On physical exam, there is usually a palpable defect in the tendon, in 75% of patients.
Up to 25% of tendon injuries can be missed when only clinical assessment is used for diagnosis.
Simmonds/Thompson test: the patient lies face down with feet hanging off the edge of the bed. If there is no plantar flexion of the foot on squeezing the calf, then there is likely rupture of the Achilles tendon.
O’Brien test: insert 25-gauge needle at right angle through the skin of calf muscle just medial to midline at a point 10 cm proximal to superior border of calcaneus. The needle should be within the substance of the tendon. Movement of the needle in a direction opposite that of the tendon during passive extension and flexion of the foot confirms an intact tendon distal to the level of needle insertion.
Copeland test: the patient is prone with the feet hanging off of the exam table. A sphygmomanometer is placed around the calf with the foot in plantar flexion and inflated to 100 mm Hg. If the tendon is intact, then extension of the foot will lead to a pressure increase to 140 mm Hg. If the tendon is ruptured, then the pressure does not change.
IMAGING
Imaging is always recommended when there is clinical concern for Achilles tendon rupture.
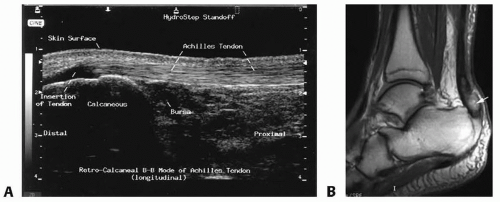
FIG 2 • A. Normal Achilles ultrasound image. B. Ankle MRI (T1-weighted image) showing a distal Achilles tendon rupture. (From Labib S. Open Achilles tendon repair. In: Wiesel S, ed. Operative Techniques in Orthopaedic Surgery. 2nd ed. Vol. 4. Philadelphia, PA: Wolters Kluwer Health; 2015:4967-4973.)
Ultrasound is a useful first-line imaging technique, with sensitivity of 100% (FIG 2A).
Ultrasound tendon gap greater than 4 mm with patient in equinus (plantar flexion) indicates the need for surgical repair.
Ultrasound can differentiate partial vs complete tear:
This is more difficult with a tear at the proximal musculotendinous junction, in which sensitivity is much lower.
MRI is the best imaging modality for Achilles tendon rupture, with sensitivity of 100% (FIG 2B).
MRI should always be obtained if any uncertainty exists regarding location, completeness, or length of tear.
DIFFERENTIAL DIAGNOSIS
Achilles tendon peritendinitis
Gastrocnemius tear or strain
Calcaneus fracture
Posterior tibialis tendon injury
Posterior tibialis stress syndrome
NONOPERATIVE MANAGEMENT
Nonoperative treatment of Achilles rupture is only an option in cases of acute rupture, with immediate diagnosis.Related posts:
 Fasciotomy of the Thigh, Lower Leg, and Foot
Fasciotomy of the Thigh, Lower Leg, and Foot
 Bony Reconstruction of Foot and Ankle (Bone Grafts)
Bony Reconstruction of Foot and Ankle (Bone Grafts)
 Vascular Reconstruction of Lower Extremity, Foot, and Ankle
Vascular Reconstruction of Lower Extremity, Foot, and Ankle
 Soft Tissue Coverage of Lower Leg—Soleus Flap
Soft Tissue Coverage of Lower Leg—Soleus Flap
 Reconstruction of Femur
Reconstruction of Femur
 Amputation of the Lower Extremity: Above-Knee Amputation, Below-Knee Amputation, Through-Knee Amputation
Amputation of the Lower Extremity: Above-Knee Amputation, Below-Knee Amputation, Through-Knee Amputation

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


