Key Terms
Community-Acquired Methicillin-Resistant Staphylococcus aureus
Carbuncle
Furuncle
Dissecting Cellulitis of the Scalp
Hoffman disease
Perifolliculitis capitis abscedens et suffodiens
An abscess results from a neutrophilic host response to something perceived by the immune system to be foreign. As such, abscesses may result from endogenous material, such as keratin from a ruptured follicle or cyst, exogenous foreign material (e.g., injected drugs, suture material), or infectious organisms (e.g., bacteria, fungus, protozoa).
Important History Questions
How long has the abscess(es) been present?
An abscess may result from an acute event (e.g., ruptured epidermoid cyst), whereas other abscesses may be recurrent (e.g., recurrent furunculosis), or even chronic in nature (e.g., hidradenitis suppurativa).
Do you have any underlying medical conditions?
Immunocompromised patients (e.g., those with HIV infection) are more likely to develop abscesses due to infections. Other conditions, such as end-stage renal disease, and visitation to dialysis centers are associated with methicillin-resistant Staphylococcus aureus (MRSA).
Have you recently traveled outside of the country?
This question is a hunt for so-called zebras that might be causing the abscesses (e.g., tropical parasites—myiasis, tungiasis) but also a quick survey for risk factors associated with more germane processes. For example, simply being a traveler, or even being in contact with travelers, is a risk factor for MRSA.
Are you currently taking antibiotics?
In a patient taking an antibiotic, when the condition has not responded or is progressive, there should be prompt consideration of culture and susceptibility studies, a switch in antibiotics, or even reassessment about whether the process was truly infectious in the first place.
Does anyone else in the family have similar lesions?
An affirmative response could indicate an infectious cause—multiple family members with methicillin-sensitive S. aureus (MSSA) or MRSA—or could suggest a common exposure among family members (e.g., myiasis, tungiasis).
Important History Questions
How long has the abscess(es) been present?
An abscess may result from an acute event (e.g., ruptured epidermoid cyst), whereas other abscesses may be recurrent (e.g., recurrent furunculosis), or even chronic in nature (e.g., hidradenitis suppurativa).
Do you have any underlying medical conditions?
Immunocompromised patients (e.g., those with HIV infection) are more likely to develop abscesses due to infections. Other conditions, such as end-stage renal disease, and visitation to dialysis centers are associated with methicillin-resistant Staphylococcus aureus (MRSA).
Have you recently traveled outside of the country?
This question is a hunt for so-called zebras that might be causing the abscesses (e.g., tropical parasites—myiasis, tungiasis) but also a quick survey for risk factors associated with more germane processes. For example, simply being a traveler, or even being in contact with travelers, is a risk factor for MRSA.
Are you currently taking antibiotics?
In a patient taking an antibiotic, when the condition has not responded or is progressive, there should be prompt consideration of culture and susceptibility studies, a switch in antibiotics, or even reassessment about whether the process was truly infectious in the first place.
Does anyone else in the family have similar lesions?
An affirmative response could indicate an infectious cause—multiple family members with methicillin-sensitive S. aureus (MSSA) or MRSA—or could suggest a common exposure among family members (e.g., myiasis, tungiasis).
Important Physical Findings
Is the abscess solitary or multiple?
This is an important physical finding because some conditions are more likely to yield singular abscesses (e.g., ruptured epidermoid cyst), whereas other conditions are more likely to yield multiple abscesses (e.g., hidradenitis suppurativa, recurrent furunculosis).
What is the distribution of the abscesses?
Some abscesses have characteristic distributions. For example, hidradenitis suppurativa occurs in the axillary and groin folds, and dissecting cellulitis occurs on the scalp. Moreover, some infectious processes occur in characteristic locations. Gram-negative bacterial abscesses are more likely to occur in the anogenital region, whereas organisms introduced from the environment (e.g., tungiasis, deep fungal infections) are more likely to occur at acral sites because traumatic inoculation is usually the source of the infection.
Does the abscess demonstrate significant associated erythema or edema?
The presence of erythema, particularly with edema, could indicate an inflammatory host response to the inciting agent but also raises concern for secondary cellulitis, which may affect treatment.
Is the patient febrile?
The presence of fever may implicate an infection. Furthermore, a significant or marked fever could alter management, necessitate use of empiric antibiotics, or even require admitting the patient to the hospital.
Furuncle
ICD10 code L02.1 to L02.9 (site-dependent)
BACTERIAL INFECTION
Community-acquired MRSA (CA-MRSA) may present with abscesses, abscesses with cellulitis, or as cellulitis alone. Management of CA-MRSA infections is not standardized, but a reasonable approach is as follows.
Healthy Patient With Abscess, With or Without Cellulitis
- •
Carry out incision and drainage.
- •
Culture for organism and sensitivity.
- •
Institute empiric antibiotic therapy (e.g., cephalexin, cefdinir, dicloxacillin, amoxicillin-clavulanate).
- •
Change to appropriate drug based on culture and sensitivity results.
Unhealthy Patient, High Index of Suspicion for CA-MRSA, and Abscess With or Without Cellulitis, or High-Endemicity Area
- •
Carry out incision and drainage.
- •
Culture for organism and sensitivity.
- •
Institute empiric antibiotic therapy with trimethoprim-sulfamethoxazole ± rifampin, minocycline-doxycycline ± rifampin, or clindamycin ± rifampin.
- •
Change to appropriate drug based on culture and sensitivity results.
Severe Infection With High Index of Suspicion for CA-MRSA
- •
Carry out incision and drainage.
- •
Culture for organism and sensitivity.
- •
Treat initially with intravenous vancomycin.
- •
Change to appropriate drug based on culture and sensitivity results.
Pathogenesis
Furuncles (boils) represent a follicle-situated infection caused by lipase-producing strains of S. aureus that break down lipids derived from the sebaceous glands. Strains of CA-MRSA are increasingly prevalent, and CA-MRSA is more likely to present as a furuncle with surrounding cellulitis. Less often, furunculosis is caused by other bacteria, such as streptococci and gram-negative organisms.
Clinical Features
- •
Furunculosis may occur at any age.
- •
Lesions may be solitary or multiple.
- •
Furunculosis may occur on any hair-bearing surface.
- •
The primary lesion is a painful, follicle-based nodule ( Fig. 13.1 ) that becomes a red fluctuant abscess ( Fig. 13.2 ) that drains purulent material spontaneously or with incision and drainage ( Fig. 13.3 ).

Fig. 13.1
Patient with an early furuncle presenting as a tender erythematous nodule that is not yet fluctuant.
(From the William Weston Collection, Aurora, CO.)

Fig. 13.2
Patient with a developed fluctuant furuncle that has started to point as a pustule on the central hair follicle.

Fig. 13.3
Patient with an older furuncle that has spontaneously ruptured, demonstrating yellowish pus.
- •
Some cases demonstrate surrounding erythema and induration indicative of associated cellulitis ( Fig. 13.4 ).

Fig. 13.4
Patient with a large furuncle of the nipple, with marked erythema, raising the possibility of CA-MRSA or cellulitis.
(From the Fitzsimons Army Medical Center Collection, Aurora, CO.)
- •
A carbuncle is simply a larger lesion that is caused by the confluence of adjacent infected follicles.
Diagnosis
- •
A presumptive diagnosis is made based on clinical findings, as supported by results of a Gram stain.
- •
The diagnosis is more fully established based on the results of culture and sensitivity studies of purulent debris and/or the anterior nasal vestibule.
Treatment
- •
Incision and drainage of singular abscesses is most often adequate therapy, even for CA-MRSA strains.
- •
Initial antibiotic therapy is based on the clinical situation (see box) but often includes cephalexin, dicloxacillin, and/or amoxicillin-clavulanate.
Clinical Course
Most cases of furunculosis are self-limited and will resolve, perhaps with some scarring or dyspigmentation. About 10% to 20% of patients will develop recurrent furunculosis.
Mycobacterial Furunculosis
ICD10 code A31.1
BACTERIAL INFECTION
Pathogenesis
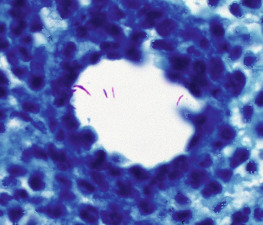
Atypical mycobacteria (AMB), including Mycobacterium marinum , Mycobacterium fortuitum , and Mycobacterium chelonae ( Fig. 13.5 ) can produce boil-like lesions in the skin. These AMB are ubiquitous in nature and are often found in soil, water, and decaying organic matter. AMB can be acquired through accidental breaks in the skin, surgical procedures, and even via pedicures or water baths. Although AMB infections may present initially as one or more follicle-based lesions, the condition may progress to a sporotrichoid pattern (see Chapter 18 ). Many AMB species common to dermatology are so-called rapid-growing species.