Abdominoplasty is the fifth most common cosmetic plastic surgery procedure performed in the United States and combining it with other procedures has become more the norm than the outlier. Liposuction is the most common adjunctive procedure, followed by breast surgery, lower back lift, and thigh lift, in addition to hernia repair and gynecologic procedures. The goal of these combination procedures includes creating more global aesthetic improvement while protecting patients from complications, based on consideration of confounding medical variables and increased risks presented by surgery of prolonged duration and exposure.
Key points
- •
Abdominal contouring surgery as a combination procedure is common, and driven by deformities resulting from issues that systemically impact individuals, including aging, weight loss, and pregnancy.
- •
Breast surgery is often performed at the time of abdominoplasty; combining breast surgery and abdominal surgery must take opposing forces of lift into consideration.
- •
Body lifts including lower back lift and thigh lift are often performed in conjunction with abdominoplasty as a lower body lift for individuals with aged, lax tissues or for individuals who have sustained massive weight loss.
- •
Combination procedures may be safely performed, with a focus on efficiency in the operating room, limiting blood loss and hypothermia, and attending to potential need for venous thromboembolism prophylaxis.
Introduction
Abdominoplasty is one of the top 5 cosmetic plastic surgery procedures performed in the United States. Many individuals consult with a plastic surgeon for abdominal contouring needs related to lax, redundant skin, stretch marks, abdominal muscle laxity, umbilical deformities, and unsightly scars. Pregnancies, abdominal surgeries, aging, and significant weight loss are causes for presentation and result in more global contour issues extending beyond the abdomen alone.
Abdominoplasty is therefore often requested and performed in combination with surgery on other body regions. The abdomen serves as a central focal area, stimulating interest in addressing adjacent areas for more global improvement. In our published series of patients undergoing body contouring for weight loss, abdominal improvement was the most prevalent reason for presentation, with 92% of patients in our series undergoing abdominal surgery, often in addition to other procedures. Abdominoplasty may be combined with breast surgery, particularly for women who are post partum, for men with gynecomastia, or for men and women who have sustained massive weight loss through diet or bariatric surgery. Abdominoplasty is also often combined with surgery on the lower back and/or thigh regions, defined as belt lipectomy and lower body lift, for individuals who have lost significant weight or have lax tissues related to aging and sun exposure. Abdominoplasty is most commonly performed with liposuction, including contouring of the back, waist, and upper and lower extremities. Fat transfer to the buttocks and breast has gained increasing popularity in combination with liposuction and abdominoplasty. Abdominoplasty also may be combined with intra-abdominal procedures such as hernia repair and gynecologic procedures.
Liposuction is the procedure most commonly performed in conjunction with abdominoplasty. Lipoabdominoplasty has become increasingly mainstream, with increasingly greater volumes of lipoaspirate proven to be safe. Matarasso published the circulation zones of the abdominal skin when liposuction was becoming a more popular adjunct to abdominoplasty in 1995, and this article still serves as a guide to safe liposuction performance in conjunction with abdominoplasty. In more contemporary literature, Saldanha and associates advocate for a more aggressive approach, performing liposuction of the abdominal skin, tolerated by limiting undermining of the skin between the xiphoid notch and umbilicus and with preservation of Scarpa’s fascia on the abdominal wall.
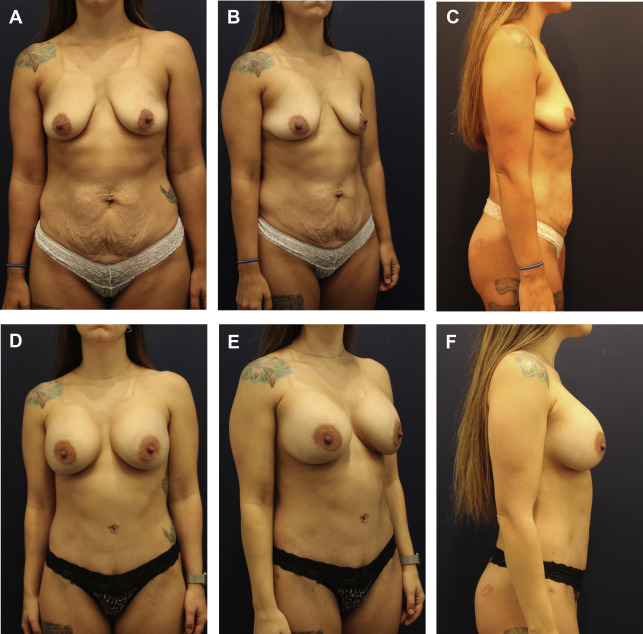
Combining cosmetic plastic surgery procedures is appealing. If there are multiple body region concerns, combining surgery allows for 1 recovery period and reduced surgical costs. The overall result can also be appreciated with 1 procedure, improving a more encompassing physical landscape, as opposed to addressing 1 area that is adjacent to another region that, left untreated, takes away from the aesthetics of the overall result. The outcome of combined surgery on adjacent areas is often more than just the sum of the parts, because each area may further enhance adjacent areas ( Fig. 1 ). There have been no formal studies on quality-of-life impact with abdominoplasty combination procedures, but it only seems logical that the outcome of safely performed combination procedures is greater than the abdomen treated in isolation. The Body Q outcomes tool will certainly aid in performance of such a study.
More extensive cosmetic plastic surgical procedures are not for everyone. Medical and surgical history must be considered. Medical comorbidities such as diabetes, cardiovascular disease, pulmonary disorders, sleep apnea, morbid obesity, and autoimmune conditions present contraindications to more complicated surgical procedures that present greater challenges to optimal recovery. Tobacco use and vaping also forecast significant healing challenges. Rather than perform combination procedures, staging may be offered to patients presenting with red flags to limit exposure to risk of one larger surgical procedure. Further, hospital-based surgery with overnight observation might be considered over ambulatory surgical center.
Overall optimization of safety is critically important. A surgical team including an experienced anesthesia provider, first assistant, and surgical technician to more expertly aid in exposure and closure help to decrease distractions, shorten procedural duration, and lessen the morbidity of a large multistage surgical procedure. Attention to positioning is critically important to avoid complications associated with nerve compression and stretch, as well as pressure issues, vascular compromise, and vision. Warming the patient with fluids, blankets, and ambient room temperature decreases the risks of anemia, wound healing issues, and infections. Prophylaxis against venous thromboembolism (VTE) is particularly important in the abdominoplasty procedure given the relatively high incidence reported in the recent plastic surgery literature. A modified Caprini scale helps to guide the choice of providing anticoagulation. Work by Pannucci and associates to more precisely determine the effective dosage of anticoagulants is ongoing. As they have described, a strict daily dosage does not necessarily provide effective prophylaxis for every patient.
Techniques in combining abdominoplasty with other procedures
Abdominoplasty and Hernia Surgery
Most plastic surgeons have trained in general surgery so they understand basic principles in straightforward hernia repair, taking techniques of plication repair of the rectus diastasis 1 step further. It is not recommended for plastic surgeons with little experience in hernia repair to perform such repairs nor is it advocated that the plastic surgeon approach incarcerated and/or complex hernia presentations if not properly schooled in such techniques. Many times hernias such as umbilical hernias and incisional hernias from laparoscopic procedures are incidentally encountered during what is expected to be a routine abdominoplasty. Repairing hernias while they are exposed assists in best care for the patient, preventing incarceration issues or a more difficult dissection in the future.
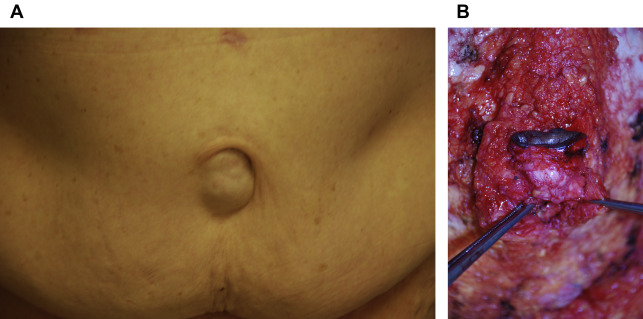
It is better to treat umbilical hernias at the time of abdominoplasty rather than at a separate setting, because umbilical hernia repair is particularly problematic if performed before abdominoplasty. As a standalone procedure, umbilical hernias are typically approached by detaching the umbilicus from the abdominal wall, repairing the hernia, sometimes with mesh, then reattaching the umbilicus after repair, leading to decreased circulation from the abdominal wall to the umbilicus. This strategy will not present a problem for later miniabdominoplasty lacking a circumumbilical incision; however, when abdominoplasty requires an incision around the umbilicus, comprising the majority of abdominoplasty cases, circulation to the umbilicus will be totally cut off with incisions under and around the umbilicus. Umbilical hernias are therefore best treated at the time of abdominoplasty. When approaching these hernias, the umbilical stalk may be incised at the most prominent location of the umbilical hernia, allowing entrance into the stalk, reduction of the hernia contents (which is almost always omentum), and closure of the base of the umbilical stalk with permanent suture to block future herniation of the omental fat ( Fig. 2 ). The incision on the umbilical stalk is closed and plication of rectus diastasis will then follow.
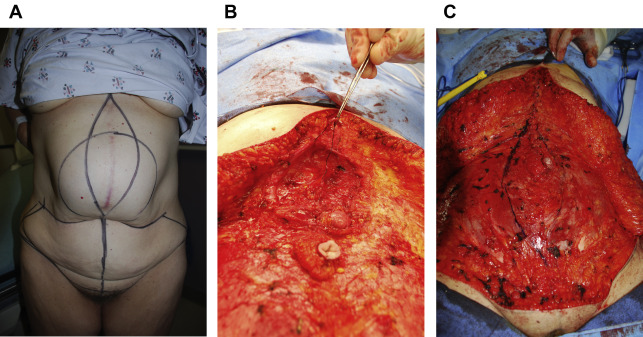
When encountering incisional and ventral hernias during elevation of the abdominal skin off the abdominal wall, the hernia must be dissected free, with reduction of hernia contents and approximation of the abdominal wall edges with permanent suture, preferably interrupted figure of 8 sutures to avoid potential unraveling of the hernia repair ( Fig. 3 ). In patients with a prior midline incision and underlying ventral hernia, excision of the midline scar and adjacent skin using a fleur-de-lis approach will improve exposure, scar, and contour outcome.
Abdominoplasty and Liposuction
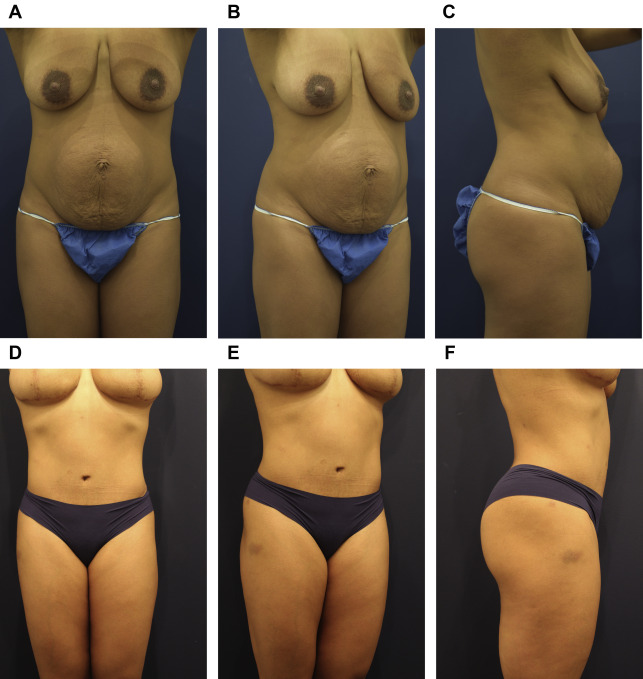
During abdominoplasty, liposuction may be performed on the upper and lower back and lateral waist to improve circumferential aesthetics of the torso, as long as the patient has good quality skin that would benefit more from deflation and subcutaneous fat reduction, and less from skin removal. Circumferential liposuction takes the result of traditional abdominoplasty to a much higher level, improving and smoothing the waist, flank, and bra line, and creating a sleeker junction with the pubis and upper thigh ( Fig. 4 ).
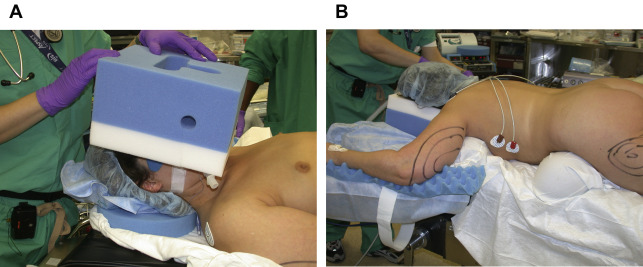
Intraoperatively, the patient is first positioned prone with careful padding, and positioning of the head and neck and arms so that liposuction may be completed on the back. Careful attention is paid to safe positioning, placing gel rolls under the upper chest/axilla and across the lumbar region. Axillary regions are supported. Arms are positioned perpendicular to the body and at the elbow. Arms and legs are placed on cushioned surfaces. The face should be placed in a prone pillow, avoiding any pressure on the eyes and maintaining the neck in neutral position. Sequential compression devices are in place and active throughout the surgery ( Fig. 5 ). Fat grafting to the buttocks might also be performed at that time if indicated.