Abdominoplasty
Alan Matarasso
Darren M. Smith
DEFINITION
Abdominal contour deformity results from relaxation of the abdominal wall and overlying soft tissues with childbearing, weight gain, aging, or a combination of the above.
Rectus diastasis is the separation of the two rectus abdominis muscles in the midline; this separation, along with stretching of the abdominal fascia, constitutes the deepest anatomical layer responsible for the abdominal contour deformity.
Lipodystrophy refers to excess adiposity, superficial to the abdominal wall, that contributes to the abdominal contour deformity.
Skin excess (most frequently present after weight loss or pregnancy) is the most superficial anatomical component of the abdominal contour deformity.
ANATOMY
The abdominal wall can be discussed in terms of three treatable tissue types, skin, fat, and muscle.
Skin (from costal margin superiorly to mons pubis inferiorly, with lateral borders defined by the anterior axillary line)
Fat in the abdominal region is either superficial or deep to the Scarpa fascia. Some surgeons aggressively excise subscarpal fat from the abdominoplasty flap, but this is not generally our practice.
The rectus abdominis muscles are a paired midline structure that must be assessed in each abdominoplasty patient to determine the need for plication.
Plication is generally indicated except in men and in the massive weight loss population.
PATIENT HISTORY AND PHYSICAL FINDINGS
Abdominoplasty patients should be low risk (eg, ASA I) healthy patients.
Abdominoplasty patients should ideally have completed their childbearing, as future pregnancy will distort the result.
Massive weight loss patients require heightened vigilance with regard to medical optimization given their unique risk profile.1
In addition to ensuring general good health in the abdominoplasty patient, special attention should be paid to venous thromboembolism (VTE) avoidance given the risk of this potentially catastrophic event after this procedure.2
In a survey of more than 1100 plastic surgeons on VTE occurrence and prevention in their practices, VTE was found to occur most frequently with abdominoplasty and abdominoplasty combined with another procedure (without a significant difference in frequency between the two).3
Thorough history taking and patient-specific risk reduction strategies based on the literature are critical in VTE avoidance.2,4
The physical exam should focus on identifying the degree to which the treatable tissues of the abdomen (skin, fat, and muscle) contribute to a given patient’s abdominal contour deformity.
Pre-existing scars should be evaluated with regard to their effect on blood supply to the abdominoplasty flap and to determine the best way to incorporate them into the incision design if they cannot be excised.
IMAGING
No preoperative imaging is routinely performed prior to abdominoplasty.
If hernias is suspected based on history or physical exam, an abdominal computed tomogram (CT) is indicated.
SURGICAL MANAGEMENT
Choice of operation from the abdominolipoplasty system of classification and treatment5 based on physical exam findings with respect to the treatable tissues of the abdomen (skin, fat, and muscle) (FIG 1):
Type I (liposuction alone): Minimal skin laxity, excess adiposity, minimal rectus diastasis
Type II (mini abdominoplasty): Mild skin laxity, excess adiposity, lower rectus diastasis
Type III (modified abdominoplasty): Moderate skin laxity, excess adiposity, lower with or without upper diastasis
Type IV (full standard abdominoplasty with or without liposuction): Severe skin laxity, excess adiposity, complete rectus diastasis
Patients can be “downstaged” to less invasive options if they cannot accept a given scar or desire minimized recovery time, but it should be explained that a downstaged procedure cannot deliver the same result as the procedure that is indicated by the abdominolipoplasty system of classification and treatment.
Preoperative Planning
Several red flag patient characteristics emerged from our experience that apply to combining abdominoplasty with any procedure.
Pulmonary conditions, history of or propensity for VTE, cardiac insufficiency, peripheral vascular disease, hypertension, obesity, bleeding diathesis, smoking, exposure to secondhand smoke, and diseases affecting microcirculation (diabetes, lupus, chronic fatigue syndrome) should be investigated and dealt with prior to abdominoplasty.
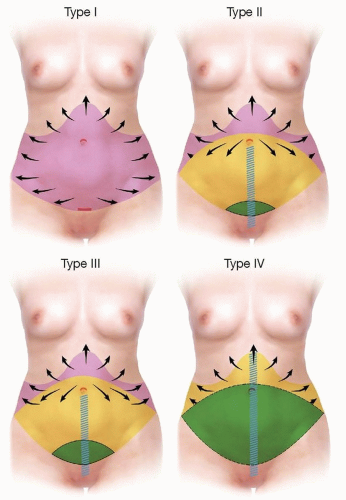
FIG 1 • The abdominolipoplasty system of classification and treatment. Type I, liposuction alone. Type II, mini abdominoplasty. Type III, modified abdominoplasty. Type IV, full standard abdominoplasty with or without liposuction. Types I and II are limited abdominoplasties. Pink, suctionassisted lipectomy; yellow, undermining; green, excision; blue crosshatching, fascial plication; arrows, transitional area.
A history of surgical site infections (especially involving methicillin-resistant Staphylococcus aureus [MRSA]) should also be addressed.
With regard to VTE prevention, our patients discontinue the use of all female hormones (including drug-eluting patches and intrauterine contraceptive devices) and nicotine in the preoperative period. They are offered prothrombogenic blood test screening and postoperative venous Doppler testing.

FIG 2 • The Miami beach chair position. The surgeon must verify that the operating table can reach full flexion prior to beginning the case.
Those at high risk for VTE based on history (Rubin’s group offers a good review of criteria with which to assess historical risk6) are referred for hematologic workup.
All of our patients are liberally hydrated and placed in compressive stockings and sequential pneumatic compression devices prior to the induction of anesthesia.
A history of surgical site infection (especially those involving MRSA) should also be addressed.
We routinely utilize nostril mupirocin ointment (GlaxoSmithKline, Research Triangle Park, NC) in the perioperative period, along with oral and intravenous antibiotics and antimicrobial body scrubs. Alcohol-based prep solutions are utilized at the time of surgery.
Positioning
Prior to surgery, it is confirmed that the operating room table can reach a full beach chair position (FIG 2).
The operation begins with the patient in the supine position.
The symmetry and angle of the arm boards is confirmed, and the arms are secured to the arm boards with a gauze wrap.
Approach
The operation is performed under systemic anesthesia (spontaneous ventilation general anesthesia, or spinal/epidural) administered by a board certified anesthesiologist in a certified ambulatory surgery facility.
A Foley catheter is inserted and thromboembolic precautions are taken as discussed above.
If multiple procedures are to be performed, the abdominoplasty is usually performed last.
TECHNIQUES
▪ Abdominoplasty
Markings
The abdominoplasty incision is marked with the patient wearing their preferred undergarment to ensure it covers the proposed incision.
The abdominal excision, essentially an ellipse of tissue between the umbilicus and mons pubis, is determined by assessing the ease in which the lower abdominal skin (from umbilicus to hairline) can be excised after grasping the pannus with both hands in an attempt for the fingers to touch the thumbs.Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree








