Abdominal Panniculectomy
Devra B. Becker
DEFINITION
Abdominal panniculus derives from the Latin pannus (cloth, garment), the diminutive of which is panniculus (piece of cloth).
Pannus was used to describe “wrinkled or flabby skin” by the Roman Pliny, but is distinct from the Greek panus, meaning swelling (panus inguinalis). Pannus is defined in modern usage as an abnormal layer of granulation tissue covering the eye or synovial space.
Panniculus morbidus was described in Petty and colleagues’ 1992 article that reported on eight patients who had restored function after wedge resection.1
A symptomatic panniculus can be graded by function2:
Grade I: chronic skin problems confined to the lower abdomen
Grade II: chronic skin problems around the naval or under a supraumbilical panniculus as well as an infraumbilical panniculus
Grade III: abdominal panniculus without chronic skin problem
ANATOMY
An abdominal panniculus is so defined by redundant skin of the abdomen that can have both horizontal and vertical excess.
There are three vascular zones of the abdomen as described by Huger.3
In Zone 1 (bounded craniocaudally from xiphoid to pubis and laterally by the lateral extent of the rectus sheath), the blood supply is the deep epigastric arcade.
In Zone 2 (bounded craniocaudally from a line drawn from the anterosuperior iliac spine [ASIS] to the pubis, and laterally by the inguinal creases), the blood supply is the superficial branches of the circumflex iliac and external pudendal vessels.
In Zone 3 (bounded craniocaudally by the costal margin to the ASIS and laterally extending from the lateral rectus sheath to the midaxillary line), the blood supply is intercostal, subcostal, and lumbar arteries.
Nerve supply to the abdominal wall is segmental and dermatomal, from T7-L1.
The lateral femoral cutaneous nerve from L2-L3 innervates the anterolateral thigh and travels medial to the ASIS.
The iliohypogastric and ilioinguinal nerves pierce the internal oblique muscle and travel along the external oblique muscle to provide sensation to the inner thigh and the groin and symphysis pubis.
PATHOGENESIS
Risk factors for development of abdominal panniculus after bariatric surgery include a higher pregastric bypass body mass index (BMI) and advanced age.4
NATURAL HISTORY
Symptomatic panniculitis is characterized by intertrigo that is refractory to conservative management with desiccants such as powder and topical antifungals.
PATIENT HISTORY AND PHYSICAL FINDINGS
For patients who have had bariatric surgery, the surgeon should assess the type of bariatric surgery the patient had (restrictive, or restrictive and malabsorptive), time from surgery, total weight loss, and length of time that weight has been stable.
Nutritional status should be addressed, including protein needs and any micronutrient deficiency.
History should be assessed for patient reports of functional impairment, particularly with activities that require hip flexion such a cycling or walking up stairs, intertrigal rashes refractory to conservative management with desiccants and antifungals, and back pain.
Physical exam should include inspection for scars and extent of panniculus, relationship of panniculus to the symphysis pubis, scars, abdominal striae, quality of skin, mons pubis edema and ptosis, intertrigal rashes or ulceration, intertrigal hyperchromia, vertical and horizontal excess, and asymmetry.
The abdomen should be palpated to assess for hernia, rectus diastasis, skin elasticity, and extent of subcutaneous fat (FIG 1).
Factors important to surgeons are different from factors important to insurance companies.5
Surgeons value stability of weight for 6 months, and time from bariatric surgery of 18 months, whereas insurance companies value chronic maceration of skinfolds.
There is no consensus on the most appropriate BMI at which to perform panniculectomy, but postoperative events increase with increasing BMI.
Panniculectomy can be safely combined with other procedures.
In hysterectomy, panniculectomy can decrease wound dehiscence and increase ease of hygiene6 without increasing complications,16 as well as increase exposure of the pelvis.
In cases of uterine cancer, concurrent panniculectomy can result in greater total lymph node counts.7
When combined with hernia repair, it can decrease recurrence.8
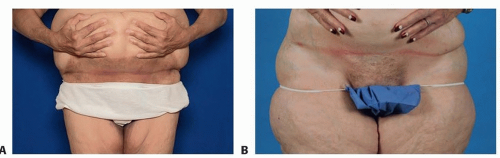 FIG 1 • Physical exam should include inspection as well as palpation. The relationship of the panniculus to the pubis should be assessed, as well as intertrigo. Photographs with the panniculus lifted help to identify hyperchromia and intertrigo. |
IMAGING
Routine imaging is not necessary in the presence of an adequate physical exam, but CT should be obtained in the case of hernia (FIG 2).
NONOPERATIVE MANAGEMENT
Nonoperative management should be aimed at improving function.
Weight loss, physical therapy for muscle rebalancing, and hygiene for intertrigo reduction are nonoperative strategies that should be trialed for several months.
SURGICAL MANAGEMENT
If the umbilical stalk is greater than 5 cm or if it is involved in a hernia, it may need to be sacrificed. Discussion of the umbilicus should be frank (FIG 3).
Blood transfusions are often not necessary, but some blood loss is expected. Transfusion rates have been reported from 9% to 12%.9
Risks of the procedure include bleeding, hematoma formation, skin flap necrosis, fat necrosis, and asymmetry.9
If a wedge excision is planned, whether the umbilicus will remain is determined based on its location cephalad to the panniculus.
The main objective of the operation is to reduce the redundant skin and subcutaneous fat inferior to the umbilicus that creates the panniculus.
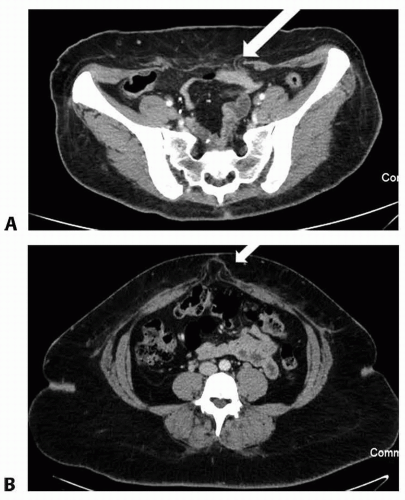
FIG 2 • CT scan can help delineate the extent of a hernia and can help with preoperative planning.
The luminal diameter of vessels is increased in obese patients, and there is some evidence that the luminal diameter remains increased with massive weight loss.
Surgeons should be mindful of the larger caliber vessels encountered in panniculectomy, even in massive weight loss patients.
The ability to close should be determined prior to resection.
Preoperative Planning
Patients are assessed by Caprini score for deep vein thrombosis (DVT) risk assessment.10
CT scans are obtained if there is clinical concern for hernia. If a hernia is present, a combined hernia repair and panniculectomy is planned.Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree








