Abdominal Hernia Reconstruction With Synthetic and Biologic Mesh
Sergey Y. Turin
Gregory A. Dumanian
DEFINITION
A hernia is a defect in at least one of the layers of the abdominal wall, permitting intra-abdominal contents such as bowel and fat to protrude past their normal confinement layer of transversalis fascia. This is in contradistinction to a bulge, which is an imbalance between the outward force of the viscera and the containing force of the intact abdominal wall, as seen in denervation injuries or rectus diastasis.
We will focus on the treatment of incisional hernias in this chapter—hernias due to a defect in the repaired abdominal wall after a prior laparotomy.
ANATOMY
The key in a hernia defect is the disruption of the continuity of the abdominal wall—depending on the etiology of the hernia and the patient’s surgical history, this may be one or many layers of the abdominal wall. In incisional hernias, this often means a midline defect at the site of the previous midline laparotomy incision (FIG 1).
PATHOGENESIS
Coughing, the Valsalva maneuver, and contraction of the stomach muscles for postural stability all increase intraabdominal pressure. This pressure is normally opposed by the abdominal wall, which is a muscular and elastic organ and can provide inward force to maintain the viscera in their domain.
When one of the portions of the abdominal wall is unable to oppose the intra-abdominal pressure either due to denervation (as in a bulge) or due to discontinuity of the musculature (as in a hernia), the viscera are forced through that portion by the rest of the competent musculature. The abdominal wall functions uniformly as a pressurized cylinder, whereas sizeable hernias and bulges serve to lower intra-abdominal pressure.
The abdominal wall is muscular but also elastic. This has great bearing on the choice of reconstructive technique, in that the reconstructed muscular and fascial components must be able to stretch, so they can absorb and dampen the sharp rises in intra-abdominal pressure that come with coughing, sudden exertion, and Valsalva.
The most successful repairs occur in the most elastic abdomens, whereas a fibrotic, scarred abdominal wall that is unyielding will have more of a tendency for stitches tearing in the postoperative period. A bridging mesh (synthetic or biologic), besides its inherent inability to provide an inward force, is also inelastic and has a compliance mismatch with the intact abdominal wall, leading to a higher rate of dehiscence and suture pull-through, as shown in FIG 3.
PATIENT HISTORY AND PHYSICAL FINDINGS
A full history and physical exam is performed, with a focus on prior abdominal surgeries and the means of closure. Patients are encouraged to obtain all previous abdominal operative reports. The medical history looking for bowel dysfunction and comorbid conditions such as diabetes, cardiac anomalies, and chronic obstructive pulmonary disease is obtained.
Gestational history is important in order to ascertain if women have had their abdominal walls stretched previously.
History of weight loss, prior abdominal wall sepsis, or peritoneal dialysis is a factor that will either increase or decrease the elasticity of the abdominal muscles.
Examine the abdominal wall with the patient both standing and lying down. Attempt to reduce the hernia to assess the degree of bowel adhesions and the compliance of the abdomen.
Document the scars of previous surgeries. Evaluate rectus diastasis by watching the patient on the descent phase of a sit-up—a maneuver that clearly shows muscle separation in all but the most obese patients.
Evaluate the skin and subcutaneous tissues for scarring, excess, and wounds because this will need to be addressed for optimal closure.
Social history is necessary, as return to work issues and help at home after surgery will need to be planned in advance.
IMAGING
We routinely obtain a CT scan of the abdomen and pelvis using oral contrast to assess the layers of the abdominal wall, any implanted meshes, or biologic materials and measure the size of the defect for all major incisional hernias. If the patient has no kidney issues, we add IV contrast for an optimal study and to obviate the need to explore the abdomen at the time of hernia closure to save dissection time, limit tissue swelling, and avoid possible bowel injury.
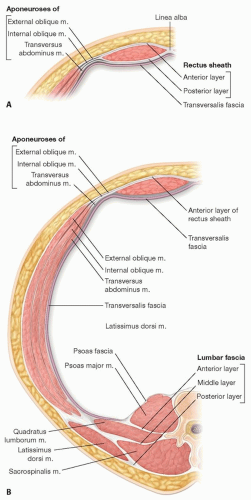 FIG 1 • A,B. Anatomy of the abdominal wall. |
NONOPERATIVE MANAGEMENT
The indications for repair of an incisional hernia are local hernia pain, a history of an obstruction, patient discomfort from an inability to raise core intra-abdominal pressure, unsightliness, and the need for intra-abdominal visceral surgery.
Small asymptomatic defects can be observed (so long as the patient is not traveling to an area lacking modern medical care), as the risk of surgery approximates the risk of observation.
For every patient, there should be a comparison of the expected benefits with the magnitude of the procedure required for repair.
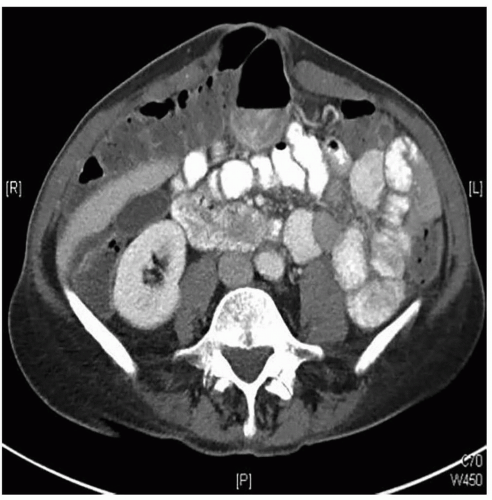 FIG 2 • CT Scan demonstrating an incisional hernia. |
SURGICAL MANAGEMENT
Preoperative Planning
These repairs are invasive procedures usually performed on an elective basis, so every patient should be optimized for surgery, including an appropriate perioperative evaluation, nutritional optimization and weight loss, and lifestyle changes such as smoking cessation.
The Caprini risk stratification model is used to assess the individual patient’s risk for DVT/PE and assign chemoprophylaxis if appropriate.
Perioperative antibiotics are routinely given for 24 hours, and topical antibiotic irrigation is used during the procedure.
The history and imaging must be reviewed and an operative plan put in place:
What incisions have been previously made? What layers of the abdominal wall are no longer continuous?
Is there mesh? If so, what kind, how large, and how was it affixed?
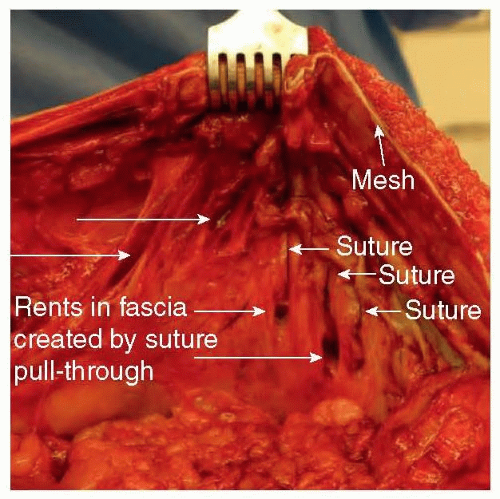
FIG 3 • Suture pull-through or “cheese wiring” due to high focal stress placed by the suture on the tissues.
Is there a concurrent procedure that needs to be performed (eg, stoma takedown or relocation or other bowel surgery)?
Assume that some level of adhesiolysis will be required, and backup plans for an enterotomy repair or bowel resection should be in place.
Positioning
The patient is in a supine position with the arms out to the sides. The field should extend from the xiphoid to pubis and down to the midaxillary line on the sides. Flank defects are repaired in the lateral decubitus position.
Approach
We use the prior incision for access into the abdominal cavity. In general, the incision must be longer than the prior scar, and so extensions into an unscarred skin are the rule.
At the end of the procedure, the prior incision, redundant skin and subcutaneous tissue, and hernia sac are excised so that healing will occur with unscarred tissue and so that the soft tissues will lie flat against the abdominal wall.
For improved aesthetics and healing, the umbilicus is removed and a neoumbilicus created (see umbilicoplasty technique in associated chapter).
TECHNIQUES
▪ Laparotomy and Development of Tissue Planes
Make a generous incision.
Enter the abdominal cavity immediately rather than trying to preserve the hernia sac. In general, start where the hernia sac is most mobile and softest, as this is where adhesions will be least. After entry into the abdomen, extend the dissection in either direction until one reaches unscarred tissue, the xiphoid, and/or the symphysis pubis.
Bowel adhesions to the hernia sac and the peritoneal surface of the abdominal wall should be widely taken down from the anterior abdominal wall, though a full abdominal exploration is not performed (TECH FIG 1).Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree








