Abdominal etching techniques are used to improve the aesthetics of the abdominal region, providing patients an athletic physique, using liposuction and fat redistribution. Based on the anatomy of fat layers, lipocontouring for deep fat liposuction and superficial fat liposculpting for superficial fat liposuction are proposed. The degree of abdominal etching is controlled by the surgeon through the extent of lipocontouring and superficial fat liposculpting. Therefore, we propose the classification of low-, medium-, and high-definition abdominal etching levels. This article offers a comprehensive description of the authors’ technique, including preoperative assessment, intraoperative procedure, and postoperative care for patients undergoing abdominal etching.
Key points
- •
Mentz first described the abdominal etching technique in the 1990s. It has gained popularity over the last 10 years with the development of new technologies and the growing ability of plastic surgeons to precisely sculpt the abdominal wall.
- •
Reciprocating power-assisted liposuction permits the complete evacuation of the deep fat compartment and allows for safe and precise sculpture of anatomic landmarks following the underlying muscular-skeletal frame.
- •
The extent of abdominal etching is offered in low, medium, or high grade of definition, and it is controlled by the surgeon depending on the amount of superficial liposuction and fat redistribution.
- •
Long-term results are maintained over time with the proper nutritional and exercising routine.
Introduction
Liposuction has become a popular procedure since the early 1980s. According to the 2018 report from the American Society for Aesthetic Plastic Surgery, the second most popular cosmetic procedure was liposuction, with more than 280,000 procedures in the United States.
Over the last 30 years, liposuction technologies have evolved, and new techniques for abdominal etching have been described. These technologies fall under five major families based on their mechanism of action: (1) suction-assisted liposuction, (2) ultrasound-assisted liposuction, (3) laser-assisted liposuction, (4) power-assisted liposuction (PAL), and (5) radiofrequency-based lipectomy. , This technological advancement permitted liposuction to be performed with fewer complication rates while improving patient safety and achieving better aesthetic results. These improvements have contributed to the positioning of liposuction as one of the most popular aesthetic procedures and have made it a more attractive option for patients seeking to improve their physical appearance, contour their figure, and achieve results that cannot be obtained solely with diet and exercise.
Abdominal etching is a group of techniques described to improve the aesthetics of the abdominal region using liposuction and fat redistribution; nevertheless, the abdominal unit cannot be aesthetically separated from the rest of the torso. Therefore, the authors recommend the treatment of the chest, abdomen, and lower back simultaneously to achieve an aesthetically pleasant and harmonic appearance. The authors have found that good surgical outcomes and postoperative profiles are achieved with the use of the PAL technology for abdominal etching ( Box 1 ). ,
- •
Faster rate of aspiration
- •
Less operator fatigue
- •
It can treat “fibrosis” in secondary cases
- •
Relative low number of complications
- •
No need for drains
- •
Fast recovery
This article offers a comprehensive description of the authors’ technique, including preoperative assessment, intraoperative procedure, and postoperative care for patients undergoing abdominal etching. Other subjects discussed include historical perspective, anatomic considerations, and complications. The content of this article assists plastic surgeons in delivering consistent and predictable abdominal etching results.
Historical perspective
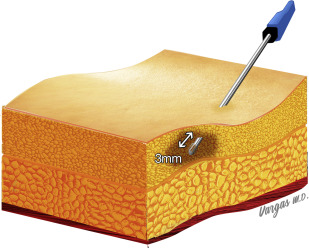
In 1977 Fisher used the term “liposuction” and described the suction-assisted lipectomy method. In 1980, Illouz introduced blunt instrumentation, which removed fat while minimizing trauma to the surrounding structures coursing between the undersurface of the dermis and the subjacent muscle fascia. In 1998, the US Food and Drug Administration approved PAL technology. This mechanically reciprocating technology (2000–4000 cpm) recreates the forward and backward motion of the operator’s arm with the cannula tip. The low reciprocating amplitude of the cannula tip (3 mm), combined with the negative pressure, allows the surgeon to precisely sculpt the superficial fat layer in addition to suctioning the deep fat layer. Under magnification, it is demonstrated how PAL is less traumatic to structures surrounding the aspirated fat.
Abdominal etching was first described by Mentz and colleagues in 1993 to enhance abdominal definition in bodybuilders. In 2007 Hoyos and Millard described the high-definition liposculpture technique with the use of vibration amplification of sound energy at resonance, and it involves several techniques that are designed to emulate athletic and attractive surface anatomy in males and females.
Anatomy of the abdominal region
To achieve a natural-looking and defined abdomen, it is of utmost importance to have a profound understanding of the anterior abdominal wall anatomy. Each layer of the anterior abdominal wall (muscles and muscle fascia, deep fat layer, superficial fat layer, and skin) has to be evaluated to achieve the desired patient outcome. Abdominal contour is substantially affected by age, genetics, muscular mass, tone, obesity, parity, and posture.
Descriptive Anatomy of the Abdominal Region
The anterior abdominal wall is limited superiorly by the costal margins and the xiphoid, and inferiorly by the iliac crests, inguinal ligaments, pubic crest, and pubic symphysis. Its lateral margins are defined by vertical lines dropped from the costal margins to the most elevated portion of the iliac crests (medial axillary line).
The linea alba extends in the midline from the pubic symphysis to the xiphoid process, and it is divided by the umbilicus into the supraumbilical and infraumbilical area. The muscular wall of the anterior abdomen is composed of the external and internal oblique, transverse, rectus abdominis, and the pyramidalis muscles.
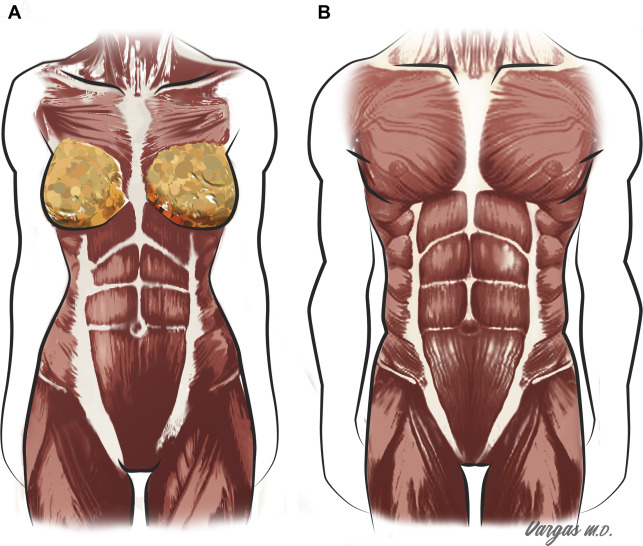
The rectus abdominal muscles consist of vertically oriented paired bellies, not necessarily symmetric, that occupies most of the central part of the anterior abdominal wall. They are separated in the midline by the linea alba and by three horizontal tendinous intersections (inscriptions). Usually, there is one pair of inscriptions at the level of the xiphoid, another around the umbilicus, and one between these two structures. There is a depression on the lateral margin of each rectus muscle that consists of the anatomic transition between the rectus muscle and the external oblique. This depression creates the linea semilunaris. , The visible shape of the anterior abdominal wall is the result of the layered osteomyofascial system, deep fat tissue, superficial fascial system, superficial fat layer, and the skin. The interactions among all these layers create the aesthetic contour through light reflection differences from prominences and shadows from depressions ( Fig. 1 ).
Adipose Tissue Layers
A profound understanding of the three-dimensional anatomy of the fat layers is key to perform abdominal etching procedures. Abdominal fat layers are practically divided into superficial and deep layers separated by the superficial fascia.
The deep adipose tissue layer lies under the Scarpa fascia (superficial fascia) and above the muscular fascia. It is composed of large, loose, and less compact fat and can often be safely aspirated without creating any significant contour irregularities.
The superficial adipose tissue layer is located between the dermis and the superficial fascia and is composed of denser, tightly adherent fat cells. Precise sculpting for abdominal etching is achieved by performing liposuction in this superficial layer. Note that above the umbilicus, most of the fat is located in the superficial layer, whereas below the umbilicus, it is found mainly in the deep layer ( Fig. 2 ).
According to the distribution of fat layers, we propose the term lipocontouring (LC) for deep fat liposuction and superficial fat liposculpting (SFLS) for superficial liposuction. It has been previously demonstrated that superficial liposuction, using proper technique, preserves the skin microvascular network of the abdominal wall.
Topographic Anatomy/Abdominal Subunits
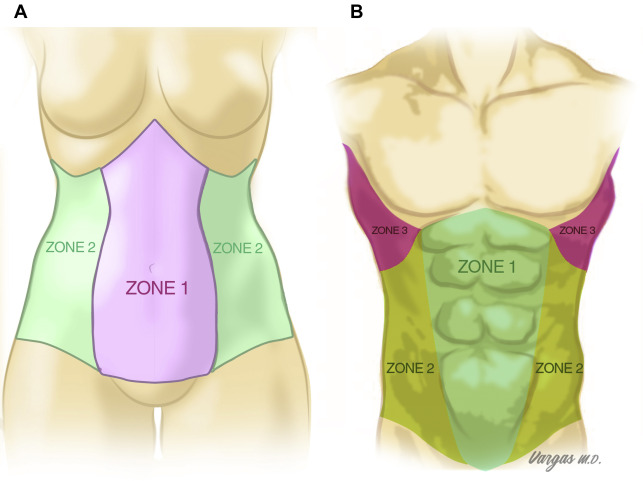
The medial abdomen (zone 1) is the area that overlies the rectus muscles bordered laterally by the linea semilunaris. The lateral abdomen (zone 2) is the territory that extends beyond linea semilunaris. This area is in continuation with the lower back posteriorly and the serratus triangle (zone 3) superiorly ( Fig. 3 ).
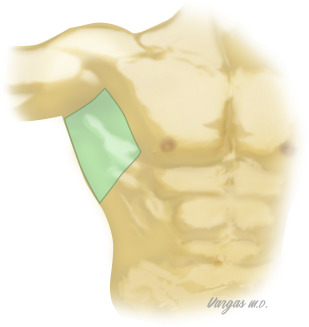
The serratus triangle (zone 3) is the area that is bordered anteriorly by the oblique lateral edge of the pectoralis muscle, posteriorly by the latissimus dorsi, overlying the serratus muscles, and in continuation with zone 2 inferiorly ( Fig. 4 ).
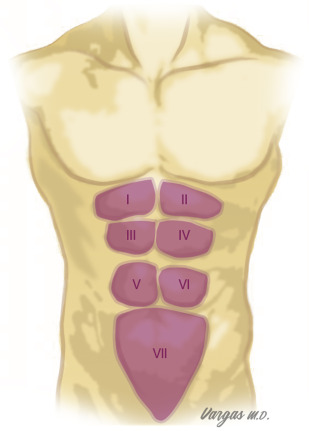
The term “six-packs” refers to the rectus muscle subunits. These bellies are separated vertically by the linea alba and horizontally by the abdominal inscriptions. The inscriptions are tendinous connections between the rectus muscle subunits with high anatomic variability. In general, the lower pair of inscriptions are located around the level of the umbilicus, whereas the highest couple of inscriptions are around the level of the xiphoid. Another pair of inscriptions is usually present between these two structures. Note that the inscriptions are almost always not perfectly symmetric and sometimes are more oblique than horizontal. The external anterior abdominal surface recreates rounded square areas that vary from six to eight subunits (I to VIII) above the umbilicus, which represent the underlying rectus bellies. Under the lowest inscription, an odd subunit is found, which is nominated either with the number VII or IX ( Fig. 5 ).