In the industrialized world, venous leg ulcers (VLUs) represent over 75% of all lower extremity ulcers and have a high incidence and prevalence in the community. It is estimated that up to 1% of the adult population have or have had a leg ulcer. The recurrence rate is as high as 50% within a year, but this risk can be cut in half with the ongoing use of compression garments. According to published data only 20% heal within less than 3 months, 50% take more than 1 year, and 20% take over 2 years, and the remaining 10% never heal.
Treatment of any medical condition first requires an adequate diagnosis. While VLUs can in general be diagnosed clinically, there is always the need to consider other etiologies and associated conditions. It is frequent in the mind of clinicians to think about two possible etiologies when it comes to leg ulcers: venous and arterial. But, unfortunately, the differential is quite broad and sometimes is not as straightforward as it may seem. The table that follows shows just a handful of conditions that may mimic a VLU. These conditions can present alone or coexist with varicosities which can lead to the incorrect diagnosis. The list is not exhaustive, but it provides a point of reference to consider ( Table 15.1 ).
Table 15.1
Conditions That May Mimic a Venous Leg Ulcer
| Infectious | Autoimmune | Hematological | Other |
|---|---|---|---|
|
|
|
|
The diagnosis of VLU is usually clinical. The typical features include:
Location: The medial aspect of lower leg is more common than the lateral aspect, but it can sometimes be circumferential and even affect the dorsum of the foot.
Pain: VLUs may or may not be painful. The traditional teaching was that VLUs were not painful and arterial ulcers were. This is not a reliable symptom, and pain may be severe in VLUs as well, mainly if there is infection present.
Associated findings: Typically there is hyperpigmentation due to hemosiderin deposits, but this is not pathognomonic of VLUs either. Any chronic inflammatory condition can potentially cause extravasation of red blood cells, causing hemosiderin deposition. Edema is commonly seen, as well as some degree of varicosities or telangiectasias. VLUs rarely go beyond the subcutaneous layer. If there is an exposed tendon, fascia, or muscle, the diagnosis is something more serious than venous insufficiency alone.
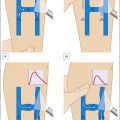
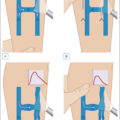
Diagnostic studies: In addition to obtaining a good history and physical examination, diagnostic studies are helpful when the diagnosis is not clear. A skin biopsy obtained from the edges of the ulcer and sent to both microbiology for cultures, including bacterial, fungal, and acid-fast bacilli, and to pathology for histological examination ( Figs. 15.1 and 15.2 ). In my practice, I like to specify the slide to be read by a dermatopathologist.
Ulcer diagnosed as venous leg ulcer turned out to be pyoderma gangrenosum of unknown origin.
Right ankle venous leg ulcer
Vascular studies, including a venous reflux Doppler, and arterial studies are performed routinely. About 30% of patients with VLU also have coexisting peripheral vascular disease, which would need to be addressed first before being able to offer compression therapy for the venous component. A frequent problem identified when ordering venous reflux studies is the fear of the ultrasound technologist to scan over the ulcer area, missing valuable information such as the presence of incompetent perforators responsible for the formation of the VLU. I typically provide the patient with a prescription for a lidocaine-prilocaine cream to be applied to the ulcer site prior to the ultrasound and covered with a film dressing, such as a Tegaderm film dressing, so that the technician can freely scan over the ulcer site without causing pain or exposing the ulcer to contamination with the ultrasound probe. I also make the patient aware of the study being conducted and to ensure that a true “reflux study” is conducted, as many times Dopplers are done with the goal of diagnosing or ruling out a deep venous thrombosis without looking at the functional aspects of the study.
Microbiology: Traditional cultures offer limitations, as frequently skin ulcers can be colonized or infected by multiple microorganisms. It has been customary practice from microbiology labs to consider samples containing more than three different microorganisms as contaminated, and in this case no sensitivities are run. In real life there is no law in nature that precludes multiple different microorganisms from simultaneously infecting a lesion that is exposed to the elements. This problem can be solved using DNA sequencing or PCR analysis, which offers multiple advantages, including the possibility to detect bacteria in biofilm and bacteria that may not grow in culture media or under the conditions of the incubation system employed by the laboratory. Nowadays these techniques can also provide helpful information regarding the presence of genes that induce antibiotic resistance, making the selection of antibiotics more appropriate.
Treatment
There are universal interventions utilized in all sorts of ulcers that include the following elements:
-
1)
Cleansing
-
2)
Wound bed preparation
-
3)
Dressing
Cleansing: the cleansing agent of choice should be noncytotoxic. In my practice, my preferred options include hypochlorous acid (Vashe) or a 0.25%–0.5% acetic acid solution. Hypochlorous acid solution can be obtained over the counter, while acetic acid solution requires a prescription. An inexpensive alternative is to have the patient prepare the solution at home by mixing six tablespoons of white kitchen vinegar in one liter of boiled or bottled water ( Table 15.2 ).
Table 15.2
Factors That Contribute to Lack of Healing
| Internal | External |
|---|---|
|
|
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


