9 Improving the Quadrantectomy Defect
Aesthetic resections and attention to parenchymal closure have recently been advocated to avoid poor cosmetic results after large quadrantectomies. Several techniques of partial breast reconstruction, such as flaps or reduction mammaplasty procedures, 1 – 3 have been proposed; however, these require training in reconstructive plastic surgery. Most T1 and small T2 tumors can be managed without mastering such elaborate plastic surgery procedures. In these cases the final outcome can be impaired because of unfavorable and visible scarring, asymmetry of the areolas, localized glandular defects, or asymmetry of breast volume. 4
In this chapter, we present several surgical approaches for improving the final cosmetic result of breast-conserving treatment. These techniques refer to the level 1 oncoplasty defined by Clough. 5 Surgical techniques allow the removal of a large tumor, avoiding the mastectomy, and decrease the occurrence of involved margins. 6 Oncologic results of conservative treatment with oncoplasty techniques confirm the good results. 7
Surgical Technique
Preoperative Markings
The day before surgery, the surgeon must discuss with the patient the planned surgical approach and the final location of the scars. The breasts are analyzed with the patient in the standing position, and any asymmetry of breast shape, size, or areolar position should be noted and discussed with the patient.
Asymmetry may be caused by increased breast volume from the tumor or residual edema or hematoma after previous biopsies. Such asymmetry should be distinguished from congenital asymmetry.
The result will be better in women with large breasts than in women with smaller breasts. This information should be discussed with the patient.
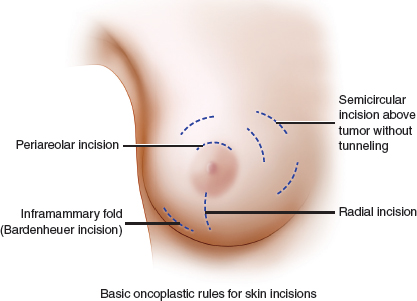
The midline should be marked between the breasts and inframammary folds. These markings are used to assess symmetry after the operation. The planned skin incisions are drawn in permanent marker with the patient still standing. There is general agreement among breast surgeons that radial incisions are performed in the lower middle part of the breast and circumareolar incisions in the upper middle part.

This patient shows good scar positioning, with asymmetry of the NAC.

This patient’s postoperative results after right breast radiotherapy are satisfactory. The left NAC was relocated.

A circumareolar incision in the inferior quadrants could create a disfiguring crease between the areola and the inframammary fold. A radial scar in the upper part of the breast may be too visible if it exceeds the décolleté line. This patient shows poor results, because the radial scar is evident in the décolleté area and the external position of the NAC.
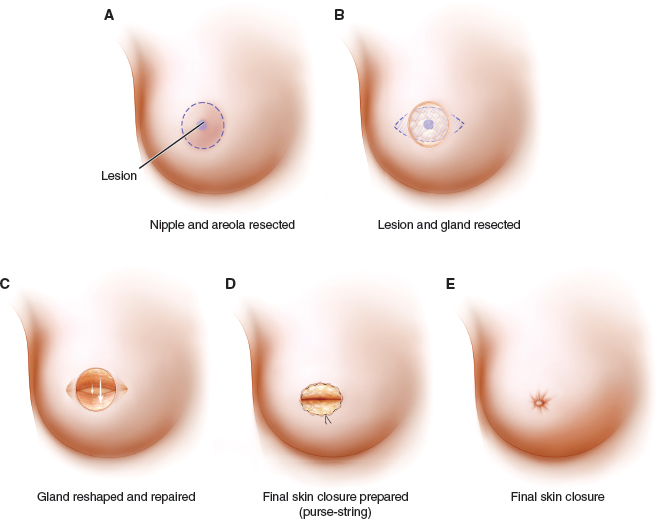
Periareolar 5 incisions provide good results if the tumor is located close to the areola; otherwise extended skin undermining can leave disfiguring skin retractions. Subareolar tumors can be performed by periareolar excision of the NAC and tumor, with purse-string closure and glandular plication (A through E). When the tumor is located in the upper outer quadrant, a radial scar allows good exposure of the tumor site, but it is recommended that the scar be lowered to avoid crossing the décolleté line. If the scar must extend toward the axilla for lymph node dissection, using a broken line is suggested to decrease scar contraction and skin retraction.
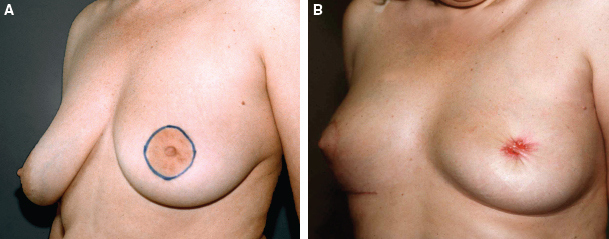
This patient had a central tumor (A). She is shown after a central quadrantectomy with a glandular defect, skin undermining, gland closure, and purse-string skin closure (B).

The need for skin resection generally depends on the possible connection between the tumor and the dermis, especially tumors located superficially in the gland. When the tumor is deeper within the glandular tissue, an inframammary incision works well.
The marking should be made 1 cm above the inframammary fold to ensure that it will not be visible under the bra. The length of the incision should be 5 to 6 cm but can easily be extended toward the axilla to perform a sentinel node biopsy or complete node dissection. An inframammary incision with extensive undermining of the breast allows the surgeon to explore the whole breast and remove a tumor in any quadrant, without modifying the breast’s shape. The patient shown here underwent a radio-active, probe-guided tumorectomy using a retroglandular approach and an inframammary incision.
Related posts:
 6 Breast-Conserving Therapy: Decision-Making and Anticipating the Unfavorable Aesthetic and Functional Result
6 Breast-Conserving Therapy: Decision-Making and Anticipating the Unfavorable Aesthetic and Functional Result
 10 Breast Radiotherapy in Oncoplastic Surgery
10 Breast Radiotherapy in Oncoplastic Surgery
 11 Indications and Benefits of Oncoplastic Breast Surgery
11 Indications and Benefits of Oncoplastic Breast Surgery
 8 Improving the Partial Mastectomy Deformity
8 Improving the Partial Mastectomy Deformity
 14 Psychosocial Aspects of Oncoplastic Breast Conservation
14 Psychosocial Aspects of Oncoplastic Breast Conservation
 13 Timing of the Oncoplastic Reconstruction: Immediate, Delayed, and Delayed-Immediate
13 Timing of the Oncoplastic Reconstruction: Immediate, Delayed, and Delayed-Immediate
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


