8 Improving the Partial Mastectomy Deformity
The long-term success of BCT is measured by the rate of local control and the cosmetic appearance of the conserved breast. Larger resection margins improve local control to a small degree but negatively affect the final cosmetic outcome. Studies have reported the results of breast conservation to be excellent to good in 80% of cases. 1 Most of these studies were conducted by radiation oncologists and involved self-reporting by patients. The patient selection and surgery are greater confounding factors than radiation in the overall cosmetic result of breast conservation.
The selection criteria for BCS are ill defined. In randomized trials, a small tumor size was the primary indication for BCS. 2 Large tumors in small- to moderate-sized breasts were generally treated with a total mastectomy and immediate reconstruction. Neoadjuvant chemotherapy and hormone therapy can be used to decrease the tumor size, making more patients candidates for a partial mastectomy.
A reconstruction is performed whenever the partial mastectomy causes a noticeable breast deformity. The surgical approach is determined by the size of the defect in relation to the size of the breast. Patients with small defects in large- or medium-sized breasts generally do not need reconstruction. This chapter focuses on improving the partial mastectomy deformity, without altering the nipple position or performing contralateral symmetry procedures. Resections that remove more than 15% to 20% of the breast volume require volume replacement with distant flaps or volume displacement through parenchymal rearrangement. These techniques are discussed in other chapters.
Patient Assessment
The magnitude of the parenchymal and cutaneous excision correlates directly with the cosmetic outcome. When large volumes of tissue are excised, the risk of an unfavorable cosmetic result increases. 3 , 4
The ratio of the resection volume to the breast volume is critical in the decision-making process to determine whether oncoplastic reconstruction is necessary.
Stevenson et al 5 found that excising more than 12% of the breast predicted poor cosmesis. Cochrane et al 6 evaluated 151 women undergoing breast conservation. They assessed the cosmetic outcome relative to the estimated percentage of breast volume excised. In patients in whom less than or equal to 10% of the total breast volume was excised, 83.5% were very satisfied with the results, compared with only 37% of the patients in whom more than 10% of the breast volume was excised.
Surgeons should be aware that removing medial and inferior tumors can be very disfiguring. 7

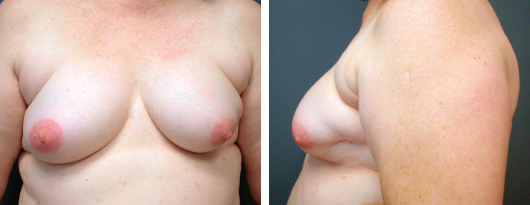
Medial defects can result in a contour deformity after a lumpectomy that is very noticeable, even if the patient is clothed.
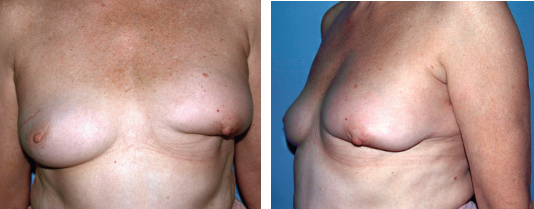
Tumor resections in the inferior quadrant can result in a “snoopy nose deformity,” with the NAC prolapsing over the excision site. This deformity is accentuated by postradiation sequelae, such as fibrosis and retraction. Removing skin at the time of a partial mastectomy distorts the nipple position, especially in the lower quadrants. Because younger women have less breast fat, the cavity that forms after the tumor resection is less likely to collapse and create a deformity. Larger breasts tolerate the removal of larger amounts of tissue without disfigurement but are more prone to the postradiation sequelae of fibrosis and retraction.
Treatment Decision-Making
The traditional approach to managing a lumpectomy or partial mastectomy defect in the United States is to close the skin over the underlying parenchymal defect. A recent review by Morrow et al 8 stated that a superior cosmetic result is usually achieved when the breast tissue is not reapproximated. This purportedly allows the breast to remodel after the resultant defect fills in with fluid. This technique is useful in larger breasts with a deep tumor location. Fluid reabsorption and scar contracture can frequently result in skin dimpling after superficial tumors are resected, particularly in smaller-breasted women with minimal breast fat.
Breast reapproximation after a partial mastectomy is often performed in Europe but has not been widely adopted in the United States. This approach can cause the nipple to deviate if the skin envelope has not been separated from the underlying breast. It can, however, help to avoid some of the breast contour deformities seen with a skin-only closure technique—lateral breast distortion, skin retraction, and deviation of the NAC toward the scar. It is especially useful in defects in the upper quadrant of the breast. The use of breast advancement flaps to close lumpectomy defects is described later.
Preoperative Planning
Box 8-1 Predictors of Residual Disease at the Time of Local Resection
Large tumor size
Nodal positivity
High tumor grade
Palpable cancer on presentation
Extensive intraductal component
Patient is younger than 45 years of age
Delineating the extent of the tumor in the breast is crucial to treatment planning. It is especially helpful to carefully review the mammogram and ultrasound results with the radiologist. A percutaneous core needle biopsy performed before the definitive treatment can provide valuable information and reduce the incidence of involved margins at the time of the resection. Bracketing guidewires are useful in guiding the surgical resection of nonpalpable lesions. Contrast-enhanced MRI scanning has improved the sensitivity of determining the tumor extent and is being studied as an adjunct in preoperative planning.
Positive margins after a lumpectomy or quadrantectomy for invasive cancer or ductal carcinoma in situ occur in up to 25% of cases. 9 Risk factors for involved margins at the time of definitive treatment include aggressive tumor biology; an extensive, noninvasive component to the tumor; and a young patient age. An intraoperative margin analysis by touch preparation cytology or frozen section histology has been shown to reduce this risk. These techniques are time consuming and expensive and can be technically difficult because of tissue artifact from fat or sampling errors. If performed properly, however, they can significantly reduce the risk of reoperation.
Choice of Incisions
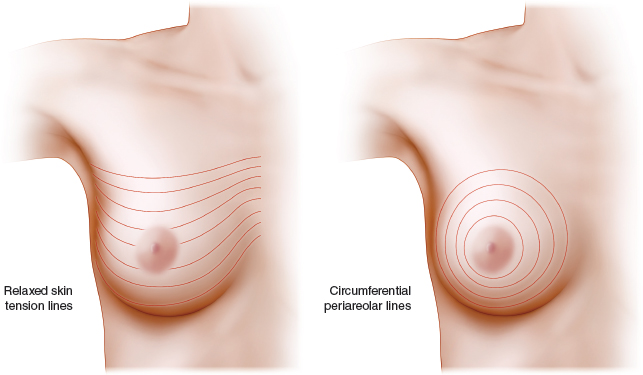
The breast incisions should be planned with the patient in the upright position in the event that a mastectomy is needed. Relaxed skin tension lines (RSTL) of the breast follow the natural wrinkle lines. Incisions within these lines generally produce the best cosmetic results. Incisions configured as concentric circles radiating from the central NAC have been advocated by many breast surgeons. These incisions are frequently perpendicular to the relaxed skin tension lines and can be disfiguring, especially in the medial quadrant of the breast.
Periareolar incisions can provide outstanding cosmesis and are especially useful if the tumor is in close proximity to the nipple-areola complex. In patients with a moderate- or large-diameter areola, these incisions can also be used to remove peripheral tumors. This approach requires a wide separation of the breast skin from the underlying parenchyma and is especially pertinent to removing benign lesions, such as fibroadenomas.
An inframammary fold incision can provide good exposure to deep tumors in the inferior pole of the breast. The breast is elevated off of the pectoralis major fascia, and the tumor is approached from underneath the breast. The incision is inconspicuous in women with moderate- to large-sized breasts. This approach is especially useful in conjunction with wire localization of nonpalpable lesions. Vertically or radially oriented incisions have been advocated to minimize nipple retraction when resecting tumors in the lower hemisphere. These incisions are especially useful in ptotic breasts with lesions located in the 9 o’clock and 3 o’clock positions. In these situations, marking the planned incision preoperatively with the patient standing is easier and ensures that incisions will be placed along the relaxed skin tension lines.
Related posts:
 6 Breast-Conserving Therapy: Decision-Making and Anticipating the Unfavorable Aesthetic and Functional Result
6 Breast-Conserving Therapy: Decision-Making and Anticipating the Unfavorable Aesthetic and Functional Result
 10 Breast Radiotherapy in Oncoplastic Surgery
10 Breast Radiotherapy in Oncoplastic Surgery
 11 Indications and Benefits of Oncoplastic Breast Surgery
11 Indications and Benefits of Oncoplastic Breast Surgery
 9 Improving the Quadrantectomy Defect
9 Improving the Quadrantectomy Defect
 14 Psychosocial Aspects of Oncoplastic Breast Conservation
14 Psychosocial Aspects of Oncoplastic Breast Conservation
 13 Timing of the Oncoplastic Reconstruction: Immediate, Delayed, and Delayed-Immediate
13 Timing of the Oncoplastic Reconstruction: Immediate, Delayed, and Delayed-Immediate
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


