9 Closed Tendon Ruptures
9.1 Extensor Indicis Proprius to Extensor Pollicis Longus Tendon Transfer
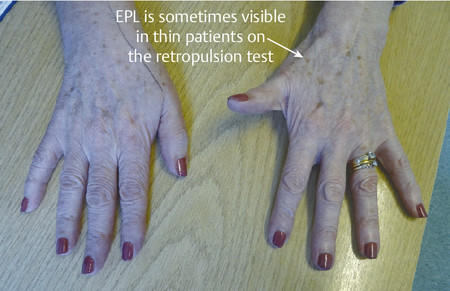
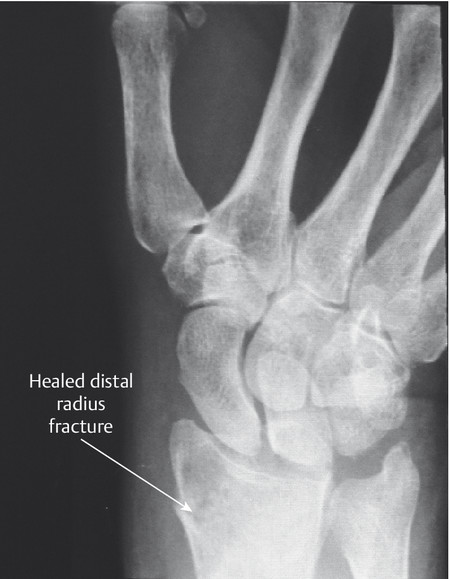
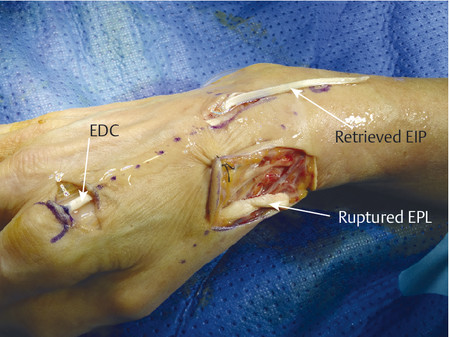
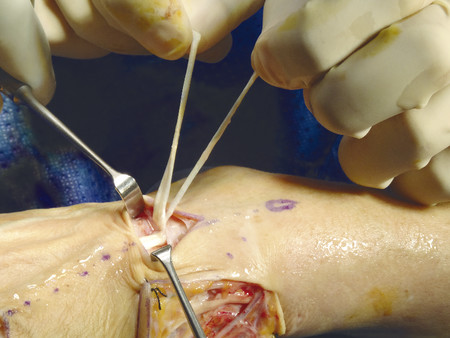
Closed rupture of extensor pollicis longus (EPL) at the wrist is the most common attrition tendon rupture. There is normally a history of distal radius fracture, often relatively undisplaced, and sometimes decades earlier. Direct repair is not possible and an extensor indicis proprius (EIP) to EPL transfer is an effective treatment.
The patient shown in Fig. 9‑1 presented to the hand trauma clinic with an inability to extend the thumb. She had been managed conservatively in cast for 8 weeks for a distal radius fracture (Fig. 9‑2). Clinical examination confirmed a ruptured EPL tendon. An EIP to EPL transfer was performed under regional anesthetic (Fig. 9‑3, Fig. 9‑4, Fig. 9‑5, Fig. 9‑6, Fig. 9‑7). The EPL which lies in the third extensor compartment is thought to undergo ischemia due to edema which consequently results in tendon necrosis and rupture.


9.2 Rehabilitation after EIP to EPL Transfer
The patient is placed postoperatively in a forearm-based splint with the repair protected in a thumb spica extension cast. The plaster of Paris splint is changed to a thermoplastic splint on day 3 and early active mobilization is started. A protective splint must be worn for 12 weeks.
9.3 Closed Flexor Tendon Ruptures
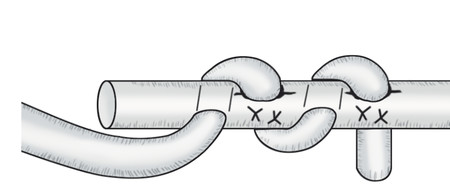
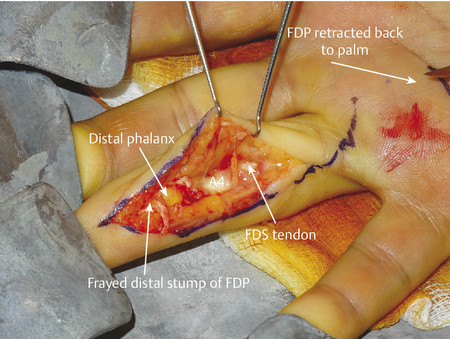
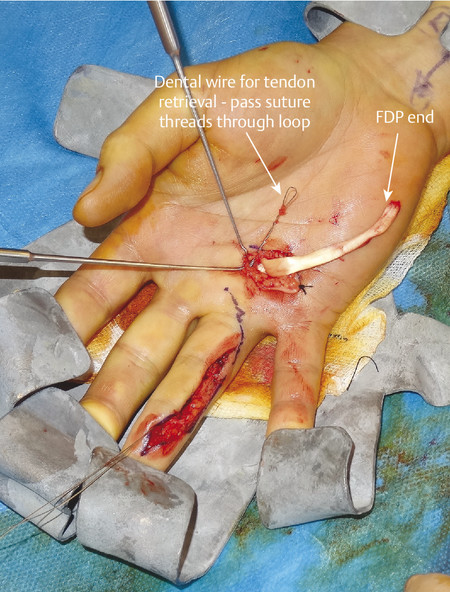
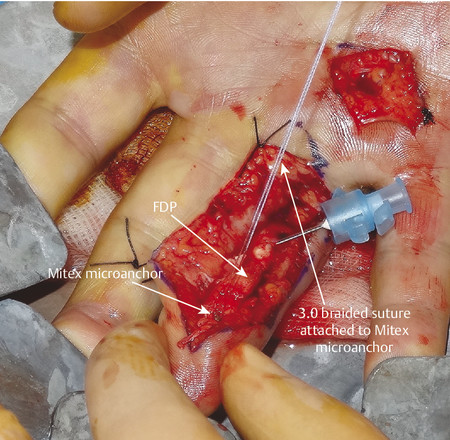
The most likely closed tendon rupture to be encountered on a hand trauma list is an FDP avulsion. The classic presentation involves the ring finger of a young rugby player who has grabbed an opponent’s shirt (jersey finger) avulsing the FDP from its insertion on the distal phalanx (Fig. 9‑8). Leddy and Packer classified these injuries into three types. In type 1, the tendon avulses from the distal phalanx and retracts to the palm, whereas in type 2, the intact vinculum longus limits retraction to the level of the proximal interphalangeal joint (PIPJ). Surgical repair of these injuries involves reinserting the FDP into the distal phalanx, which can be performed by a variety of techniques (pullout sutures, transosseous sutures, Mitek mini anchors, etc.) (Fig. 9‑9, Fig. 9‑10, Fig. 9‑11, Fig. 9‑12, Fig. 9‑13). A type 3 avulsion involves a large bony fragment attached to the FDP tendon, which is held at the distal interphalangeal joint (DIPJ) by the A5 pulley (Fig. 9‑14). These injuries can be fixed either with screws, interosseous wire fixation, or miniplate depending on the size of the bone fragment (Fig. 9‑15).





Occasionally, there can be an additional transverse fracture of the distal phalanx, which must also be fixed. This can be done either with an axial 1.1-mm K-wire, which often has to cross the DIPJ, combined with screw fixation of the fragment, or with a miniplate.
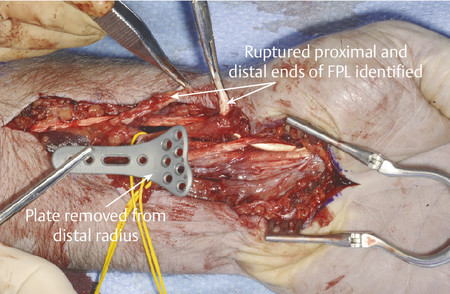
Closed tendon ruptures with less typical presentations should be carefully assessed and considered. Closed flexor tendon rupture after relatively trivial trauma, particularly in the older age group, may be due to attrition rupture at the wrist secondary to osteoarthritis or a prominent (volar) distal radial plate (Fig. 9‑16). These are seldom amenable to direct repair and require tendon reconstruction plus removal of the metalwork. An ultrasound can help determine the level of the tendon rupture, or least whether the tendon’s distal insertion is intact.
Simultaneous loss of FDP index and FPL function without a history of trauma should make the surgeon consider anterior interosseous nerve syndrome. This is thought to be secondary to neuritis (a variant of Parsonage-Turner syndrome). Here, the tenodesis test will demonstrate tendon continuity, which can be confirmed on ultrasound. Nerve conduction studies will confirm the diagnosis. The initial management is conservative, with surgical decompression only in cases demonstrating no recovery at 6 months.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


