8 Extensor Tendon Repair
8.1 Extensor Tendon Repair
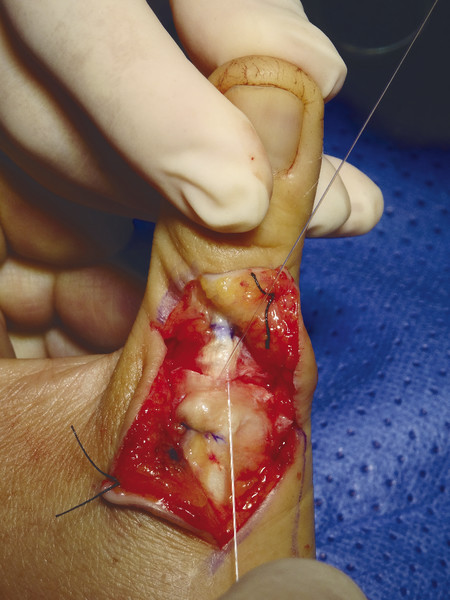
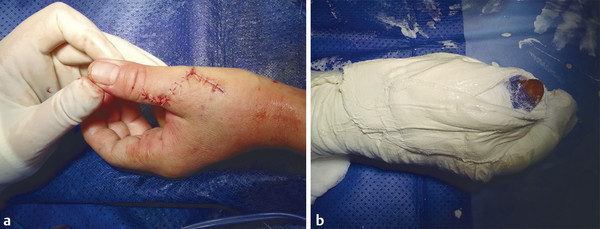
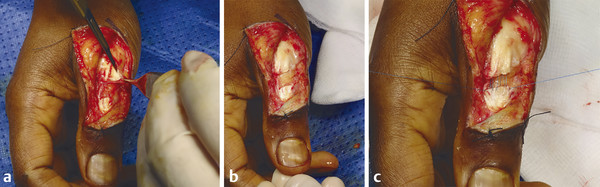
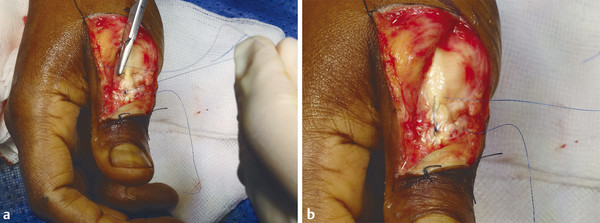
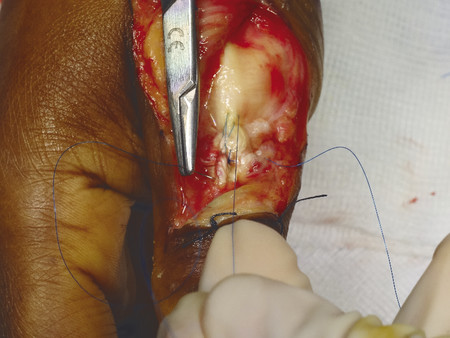
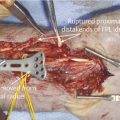
The patient presented with a glass laceration over the thumb metacarpophalangeal joint (MCPJ) and had an inability to extend the thumb on the retropulsion test (Fig. 8‑1). They were booked for local anesthetic exploration and repair of the extensor pollicis longus (EPL) (Fig. 8‑2, Fig. 8‑3, Fig. 8‑4, Fig. 8‑5, Fig. 8‑6). Most distal extensors can be done under local anesthetic; however, once you get to proximal zones 6 and 7, it can become trickier under local anesthetic as the tendons retract.


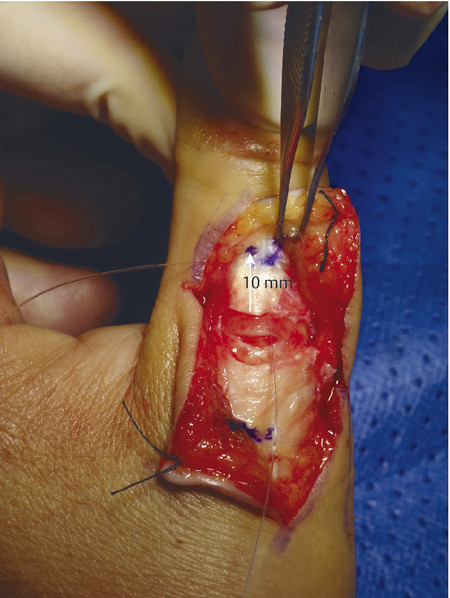
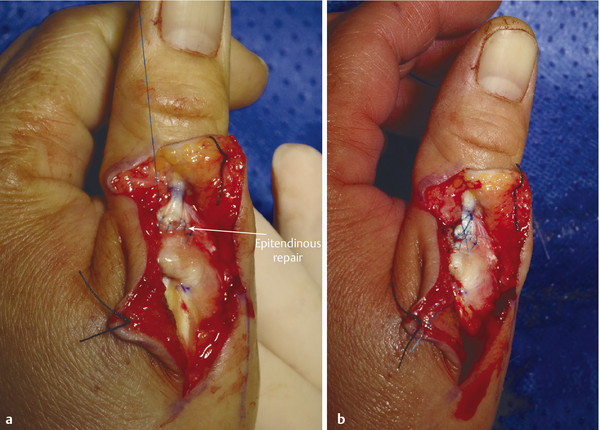
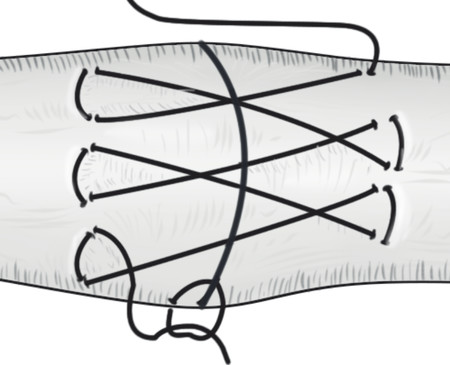
Extensor tendon injuries are more common than flexor tendon injuries due to their less protected anatomical location. Some surgeons underestimate the management of these injuries which require the same skill and attention to detail as flexor tendon surgery to avoid poor results. Verdan classified extensor tendon injuries in zones 1 to 9. The odd numbers 1, 3, 5, and 7 lie over the joints with zone 1 lying over the distal interphalangeal joint (DIPJ). The importance of this is that in zones 1 to 3 the tendon is flatter and may not easily accommodate a core stitch. Ideally, if it is possible, one should do a core repair with an additional epitendinous repair. The Silfverskiöld repair is a useful technique in flat extensor tendons and provides a strong repair (Fig. 8‑7, Fig. 8‑8, Fig. 8‑9, Fig. 8‑10, Fig. 8‑11).

Note: In zones 1 and 2, most of the proximal pull on the terminal extensor comes from the lumbricals via the lateral bands. Thus, flexing the digit at the MCPJ and proximal interphalangeal joint (PIPJ) can facilitate a tight repair by detensioning the lateral bands. Conversely, in zone 3 (and more proximally), extending the digit relaxes the proximal extensor digitorum communis (EDC) tendon to aid suture repair of the central slip.
Zone 9, which includes muscle belly, is best repaired with either Vicryl horizontal mattress sutures or a Monocryl pulley stitch.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


