Abstract
Chest contour techniques including selective fat and glandular tissue reduction have been limited in terms of inability to achieve muscular appearance in patients with very little muscular bulk in the pectoralis major musculature. Here we present our technique for achieving superior results in chest contouring using selective lipo-contouring with fat grafting.
78 Gynecomastia Excision with BodyBanking
Key Points
Gynecomastia is typically idiopathic; however, physiologic and pathological causes must be ruled out.
Minimize inferior areolar incisions, obliterate the inframammary fold, and perform near-complete excision of breast glandular tissue.
Goal is a flat chest contour with accentuation of the underlying pectoral major muscle.
Results are maximized using a combination of suction lipectomy, direct excision, along with measured structural fat grafting.
78.1 Preoperative Steps
78.1.1 Analysis
The procedure begins with a thorough preoperative analysis to identify areas of glandular and/or fatty tissue along with desired muscular enhancements and shadowing.
These areas are carefully marked preoperatively with the patient standing prior to any sedative administration.
78.2 Operative Steps
See Video 78.1.
78.2.1 Direct Excision, Access Incisions, and Suction Lipectomy
Along the inferior areolae, 3-mm stab incisions are made.
The tumescent solution (0.9% saline with lidocaine 0.1% and epinephrine 1:1,100,000) is infiltrated and given 10 minutes to take effect.
The lipectomy is then carried out using power-assisted liposuction (Power Assisted Liposuction System, MicroAire, Charlottesville, VA).
Incisions are made with a #15 blade and deepened with electrocautery, and then near-complete excision of glandular tissue is removed en bloc (Fig. 78.1).
To avoid a contour depression or “dish saucer deformity,” 2 to 3 mm of subareolar tissue is left behind in very athletic patients while 5 mm of subareolar tissue is left behind in slightly overweight patients.
Wide undermining of the inframammary is performed sharply from the inferior areolar incisions to allow excess skin to obliterate the fold and allow the skin to redrape and contract.

78.2.2 Fat Harvest, Preparation, and BodyBanking
The areas for fat harvest are determined preoperatively depending on patient’s desires and areas of lipodystrophy.
Stab incisions are made in an inconspicuous area.
The tumescent solution (0.9% saline with lidocaine 0.1% and epinephrine 1:1,100,000) is infiltrated and given 10 minutes to take effect.
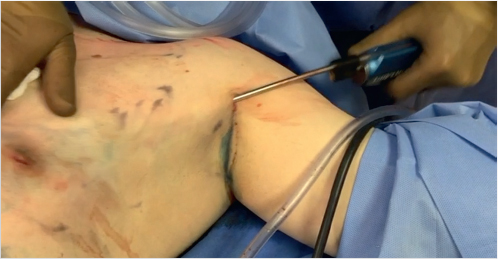
The lipectomy is then carried out using power-assisted liposuction (Power Assisted Liposuction System, MicroAire, Charlottesville, VA) or standard traditional suction lipectomy (Fig. 78.2).
The fat is drained using a metal strainer and then placed into 20-cc syringes for reinjection.
The fat is transplanted with a 1.2 Tulip fat grafting cannula (Tulip Medical Products, San Diego, CA) after dermal access of the skin with an 18-gauge needle to the superior chest to accentuate the underlying pectoral major muscle (Fig. 78.3).

Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


