Abstract
Massive weight loss patients may develop significant body deformities including severe arm ptosis due to significant volume loss with extensive skin laxity. Contouring of postbariatric patients usually requires the arm, axilla, and lateral chest wall to be addressed together as a combined aesthetic unit. Brachioplasty involves a trade-off of arm shape for scar. This book chapter reviews the preoperative, intraoperative, and postoperative treatment of severe arm ptosis.
82 Postbariatric Body Contouring: Brachioplasty
Key Points
Contouring of postbariatric patients usually requires the arm, axilla, and lateral chest wall to be addressed together as a combined aesthetic unit.
Brachioplasty involves a trade-off of arm shape for scar.
82.1 Preoperative Steps
82.1.1 Analysis
The first step is to understand the patient’s expectations and assess whether they can be met.
A thorough history should focus on weight loss, nutritional status, bariatric surgery, personal or family history of venous thromboembolic event, and smoking status. The ideal candidate should have a stable weight, preferably with a body mass index (BMI) under 30 for at least 3 months.
A detailed examination of the whole body should be performed to determine the timing and stages of the body contouring procedures. It is important to note the distribution and extent of skin laxity and adiposity in the arm, axillary region, and lateral chest wall.
To obtain adequate results, postbariatric patients usually need the arm, axilla, and lateral chest wall addressed together as a combined aesthetic unit.
82.1.2 Markings
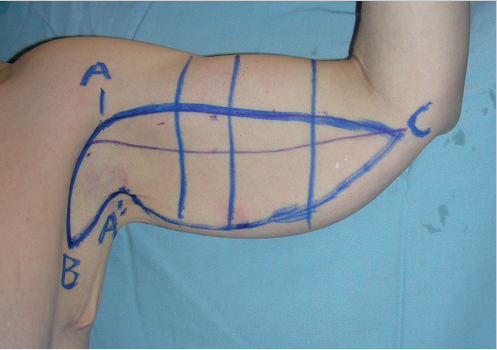
The patient is marked in the standing or sitting position with the arms abducted 90 degrees and the elbows bent at 90 degrees (Fig. 82.1).
The bicipital groove is marked to the level of the elbow (point C) and it represents the final position of the incision.
The anterior axillary line is marked along the chest.
The margins of the superior incision line are marked by placing caudal traction on the arm, with the proximal end (point A) set high in the dome of the axilla.
A pinch test is performed to determine point A’.
Points A’ and B are then connected to determine the posterior extent of axillary skin resection.
A pinch test is performed to determine the inferior line of resection.
Vertical hashmarks are drawn for alignment.
82.2 Operative Steps
See Video 82.1.
82.2.1 Positioning and Prepping
The shoulder, lateral chest wall, and arm are prepped in a sterile fashion with betadine.
The distal arm is wrapped in a sterile towel to allow full mobility during surgery. Intravenous access and monitoring devices can be attached on the forearm or the lower extremity.
82.2.2 Superior and Anterior Axillary Line Incision, and Flap Elevation
The superior and anterior axillary line markings are incised.
Dissection begins in the middle third of the incision pattern, superficial to the brachial fascia leaving a thin layer of fat on the deep fascia.
Then dissection becomes more superficial distally to avoid the medial antebrachial cutaneous nerve.
An even flap is elevated to the estimated inferior marking line (Fig. 82.2).

Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


