Abstract
The vertical thigh lift addresses the medial and circumferential thigh lipodystrophy and skin laxity following massive weight loss. It can be combined with circumferential liposuction and incorporates the relatively atraumatic avulsion of the planned resection area in order to preserve the lymphatic and neurovascular structures. This enhances healing and reduces common complications such as seroma and lymphocele formation. The scar is well hidden in the medial aspect of the thighs. Complications are typically incisional and managed with minor revision and wound care. The outcome is predictable, circumferential tightening.
84 Postbariatric Body Contouring: Vertical Thigh Lift
Key Points
Vertical thigh lift is the optimal technique to treat medial and circumferential thigh lipodystrophy, as well as skin laxity following massive weight loss.
Avulsion of the planned resection area (avulsion thighplasty) allows for maximal preservation of branching vessels, cutaneous nerves, and lymphatics that run superficial to the deep muscle fascial system in the medial thigh.
Preservation of the lymphatic and neurovascular structures enhances healing, and reduces seroma, lymphedema, and in particular lymphocele, a recognized complication of this operation.
Thorough, complete liposuction of the planned resection area accomplishes relatively atraumatic removal of skin and fat.
Vertical thigh lift can be performed as a second-stage procedure preceded by circumferential liposuction, or safely executed in combination with circumferential liposuction.
84.1 Preoperative Steps
Counsel patients about the high risk of minor wound complications and potential need for scar revision.
Determine the extent of the scar depending on the deformity and patient preference.
Perform standard preoperative laboratory analysis.
Assess nutritional status in the massive weight loss patients.
The need for coagulation tests is assessed on a case-by-case basis depending on the medical history.
No smoking for 6 weeks preoperatively and 4 weeks postoperatively.
84.2 Operative Steps
See Video 84.1.
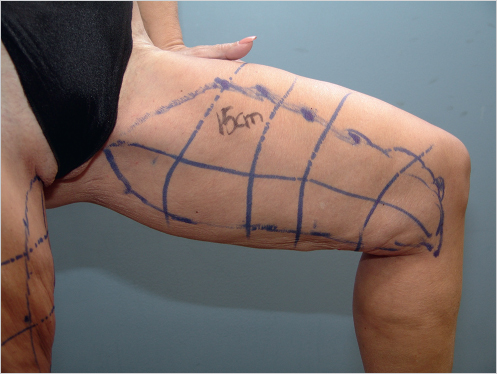
84.2.1 Markings
First, the ideal position of the vertical marking corresponding to the proposed final medial thigh incision is drawn from the pubic area to the knee, with the marking on each side being mirror image of the other.
Proximally, the marking originates at the origin of the gracilis muscle in the pubic area and extends distally as a straight line to the inferior aspect of the deformity near the medial condyle of the femur.
In patients with significant soft tissue laxity, the incision could be extended proximally into the inguinal crease or distally beyond the knee, where the linear scar is broken up at the knee area to avoid contracture.
In order to estimate the planned soft tissue resection, bimanual strong skin pinch of the redundant tissue is performed on both sides of the proposed vertical incision, and the estimated resection area is marked accordingly.
Realignment markings to ensure accurate closure are placed (Fig. 84.1).
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


