Clinical Features.
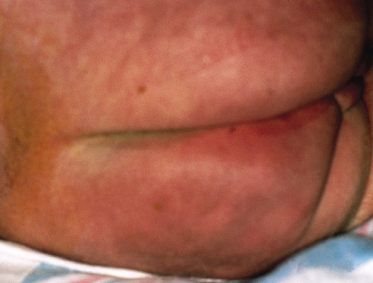
Lesions of SFN are freely mobile and not attached to deeper structures and appear in the first 6 weeks of life [9]. Affected neonates often have had perinatal asphyxia with poor American Pediatric Gross Assessment Record (Apgar) scores or difficulty with labour and delivery. Nodules and plaques are usually limited to the areas of trauma or local ischaemia, which are most commonly located on the cheeks, buttocks and posterior trunk (Figs 7.2, 7.3). The arms and legs (Fig. 7.4) can also be affected, but it tends to spare the anterior trunk and face. Occasionally, nodules can occur in the folds, mimicking lymphadenopathy [10].


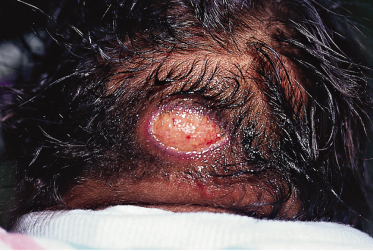
If lesions are extensive, the cutis may be fixed to deeper structures. Lesions resolve spontaneously in several weeks or persist for up to 6 months. Many calcify and are rock-hard to palpation. Ulceration may occur (Fig. 7.5), and mild atrophy of the skin may be noticed after resolution. Some nodules become fluctuant with liquefied fat. If this occurs, needle aspiration of the fluctuant material or punch biopsy can be performed to allow drainage and to prevent a nidus of infection.
Imaging with ultrasound, computed tomography (CT) or magnetic resonance imaging (MRI) may be helpful. Ultrasound images show lobulated, hyperechoic masses with increased vascularity. The CT scan shows hyperdense masses, with extension into deeper tissues. MRI demonstrates iso- or hyperintense masses on T1- and T2-weighted images with hyperintensity seen on fat-suppressed T2-weighted images [11].
Prognosis.
Prognosis is excellent, as these cutaneous lesions resolve spontaneously. Epidermal atrophy, cutaneous ulcerations and minimal scarring may occur, but these sequelae are uncommon.
Complications include hyper- or hypocalcaemia [12], nephrocalcinosis, hypertriglyceridaemia [13], hyperferritinaemia [14], lactic acidosis [15] and transient thrombocytopenia [16]. Hypercalcaemia is the most common complication. Although the cause of hypercalcaemia is unknown, hypotheses include increased intestinal calcium uptake via unregulated extrarenal production of 1,25-dihydroxyvitamin D by macrophages in the granulomatous infiltrates of the skin [17,18] or excess bone resorption caused by elevated levels of prostaglandin E [19,20].
Abnormalities of plasma lipids and lipoproteins possibly result from a peripheral oversupply of saturated fatty acids in combination with hypothermia. The role of dietary restriction of fat in such cases is unclear and probably not warranted.
Differential Diagnosis.
It is important to differentiate fat necrosis from SN, which is seen in gravely ill preterm infants and is a yellowish brawny generalized induration. These two entities can be differentiated histologically. Solitary cysts such as dermoids may also be confused with SFN, but these tend to lie in cleavage planes and are freely movable and non-erythematous. Calcinosis cutis from other causes can be ruled out by biopsy or history. Cold panniculitis results in erythematous indurated plaques 48–72 h after cold exposure. History can help to distinguish this entity. Congenital Volkmann ischaemic contracture [21,22] and large ulcerated hemangiomas [23] may be occasionally confused with SFN.
Treatment.
Therapy is usually not needed as lesions spontaneously resolve. If lesions are fluctuant, either needle or punch biopsy can drain the necrotic fat. Especially in extensive lesions, serum calcium, phosphorus, parathyroid hormone and vitamin D levels should be monitored [3] and the patient should be closely observed for symptoms such as irritability, anorexia, vomiting, constipation, renal failure or failure to thrive in the first 6 months of life.
Treatment of hypercalcaemia includes increasing renal excretion of calcium by vigorous hydration, administration of diuretics such as furosemide which waste calcium, and limiting dietary calcium and vitamin D intake. Pamidronate has been effective [24,25] but its use should be restricted to the most severe cases. Corticosteroids may effectively control hypercalcaemia by interfering with the metabolism of vitamin D to the active form 1,25-dihydroxyvitamin D. Calcitonin given subcutaneously may also be needed. In most cases, however, reassurance is the key because of the transient, self-healing nature of SFN within 6 weeks to 6 months.
References
1 Fabyan M. Disseminated fat necrosis occurring in an infant without other lesions. Bull Johns Hopkins Hosp 1907;18:349–51.
2 Mahé E, Girszyn N, Hadj-Rabia S et al. Subcutaneous fat necrosis of the newborn: a systematic evaluation of risk factors. Br J Dermatol 2007;156:709–15.
3 Norwood-Galloway A, Lebwohl M, Phelps RG et al. Subcutaneous fat necrosis of the newborn with hypercalcemia. J Am Acad Dermatol 1987;16:435–9.
4 Glover MT, Catterall MD, Atherton DJ. Subcutaneous fat necrosis in two infants after hypothermic cardiac surgery. Pediatr Dermatol 1991;8:210–12.
5 Taieb A, Douard D, Maleville J. Subcutaneous fat necrosis and brown fat deficiency. J Am Acad Dermatol 1987;16:624–5.
6 Silverman AK, Michels EH, Rasmussen JE. Subcutaneous fat necrosis in an infant occurring after hypothermic cardiac surgery. J Am Acad Dermatol 1986;15:331–6.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


