67 Scapholunate Capsulodesis
Abstract
The scapholunate interosseous ligament (SLIOL) has a stabilizing function which is critical in wrist joint biomechanics. Failure of this ligament can lead to instability and eventual degenerative changes. In cases where the ligament is not repairable, reconstruction can restore stability and diminish the likelihood of degeneration. Scapholunate (SL) capsulodesis is a surgical attempt to reconstruct the ligamentous relationship between the scaphoid and lunate using extrinsic ligamentous structures to restore stability.
67.1 Introduction
Isolated scapholunate interosseous ligament (SLIOL) disruptions can occur in isolation or as a group of more complex carpal ligamentous structures. Most of these injuries are traumatic in nature. Scapholunate (SL) capsulodesis (and capsulorraphy) is a surgical attempt to recreate the ligamentous relationship between the scaphoid and lunate. Although it can be utilized for more complex and comprehensive injuries, for simplicity of illustration, it will be discussed within this chapter and be limited to isolated SLIOL ligament injuries.
67.2 Anatomy
The carpus comprises of eight bones attached by a complex system of intrinsic ligaments. Its relationship to the remainder of the upper extremity is facilitated by an attachment of extrinsic ligaments as well. However, no tendinous insertion exists on the proximal row of the carpus, which is formed by the scaphoid, lunate, and triquetrum. The forces across this intercalary system is therefore dictated by external forces such as tendinous insertions proximal and distal to the proximal carpal row. Disruption of the stabilizing components of the proximal carpal row such as a SLIOL tear leads to derangement of the anatomic relationships between bones, with alteration of kinematics and eventual degenerative changes.
67.3 Pathophysiology, Nonoperative Treatment, and Natural History
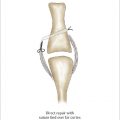
Force transmission from the digits enter the carpus mainly though the capitate and are then transmitted across the scapholunate junction. This force, by virtue of the local anatomy, will place a flexion force within the body of the scaphoid, an extension force across the lunate, and diastasis between these two bones; these deforming forces are resisted by the intact SLIOL(► Fig. 67.1).
The natural history of a SLIOL tear is “scapholunate advanced collapse” (SLAC) wrist. The dissociated carpus no longer functions as a solitary unit, resulting in abnormal carpal motions, and subsequent increases in develop pressures across the radiocarpal and midcarpal joints. Erosions of articular surfaces ensue, with the eventual development of posttraumatic osteoarthritis. 1
67.4 Clinical and Imaging Evaluation
A thorough history and physical can often elucidate and differentiate the diagnosis of scapholunate (SL) incompetence. Tenderness at the scapholunate junction and a positive Watson maneuver can especially pinpoint the pathology to this location.
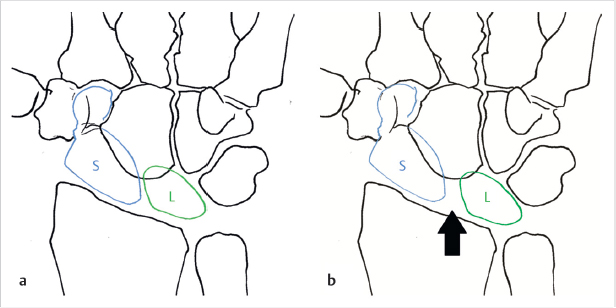
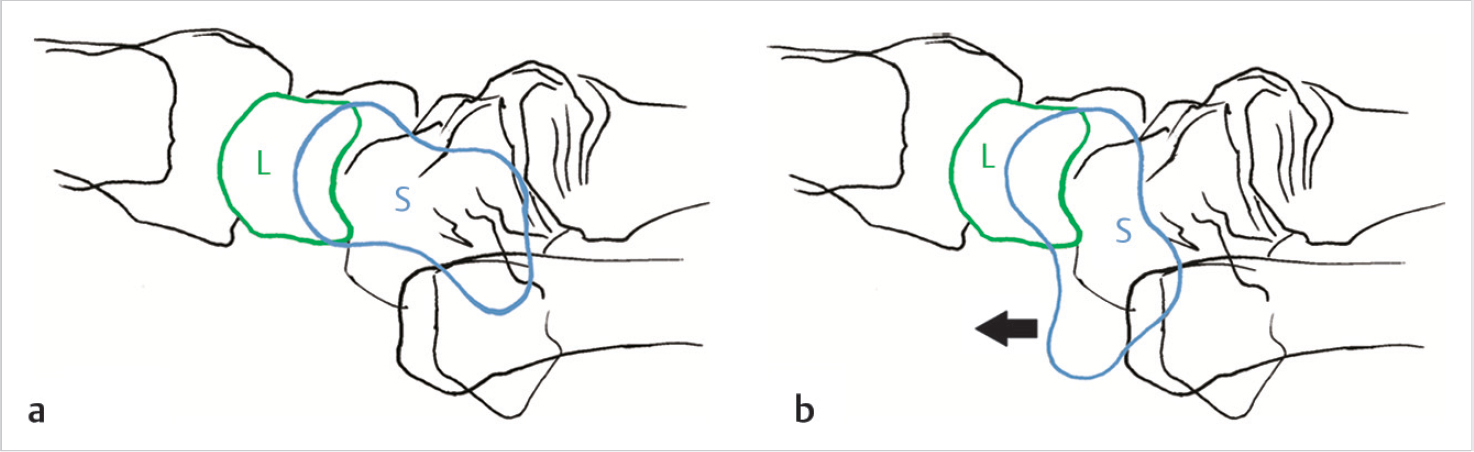
Plain radiographs in the PA, lateral, and oblique views can reveal a diastasis between the scaphoid and lunate. Greater than 3 to 4 mm gapping may offer the appearance of a “Terry Thomas sign.” On the lateral view, the SL angle is a line drawn between the long axis of the scaphoid and lunate on the lateral X-ray view. Normally, this angle measures between 30 to 60 degrees. Given the propensity of the scaphoid to flex in the absence of a competent SLIOL, the SL angle on the lateral film will be increased > 60 degrees. This is termed dorsal intercalated segmental instability (DISI) (► Fig. 67.2). Provocative radiographs such as PA clench or scaphoid X-rays can also accentuate the radiographic malalignment.
CT offers three-dimensional insight into the osseous carpal relationships; this is often helpful in complex carpal dissocia-tions and fractures. However, MRI is more useful in showing the SLIOL ligament, intrinsic and extrinsic ligaments, and associated soft tissue injuries.
Related posts:
 62 Finger (PIP/DIP) Collateral Ligament Repair
62 Finger (PIP/DIP) Collateral Ligament Repair
 65 Thumb Metacarpophalangeal Joint Collateral Ligament Reconstruction
65 Thumb Metacarpophalangeal Joint Collateral Ligament Reconstruction
 66 Scapholunate Ligament Repair
66 Scapholunate Ligament Repair
 63 Finger Metacarpophalangeal Joint Collateral Ligament Repair
63 Finger Metacarpophalangeal Joint Collateral Ligament Repair
 68 Scapholunate Ligament Reconstruction (Brunelli Types)
68 Scapholunate Ligament Reconstruction (Brunelli Types)
 64 Thumb Metacarpophalangeal Joint Collateral Ligament Repair
64 Thumb Metacarpophalangeal Joint Collateral Ligament Repair
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


