68 Scapholunate Ligament Reconstruction (Brunelli Types)
Abstract
The scapholunate (SL) ligament is a critical component of the architecture of the wrist, and its stabilizing function a cornerstone of joint mechanics. Failure of this ligament can lead to instability and eventual degenerative changes. In cases where the ligament is not repairable, reconstruction can restore stability and theoretically diminish the likelihood of degeneration. Several options for ligament reconstruction are available. We describe one type using a tendon graft.
68.1 Description
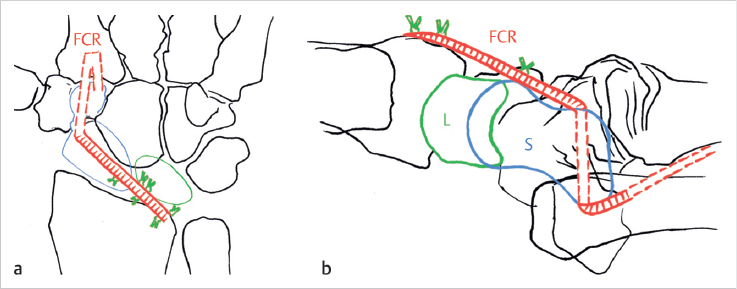
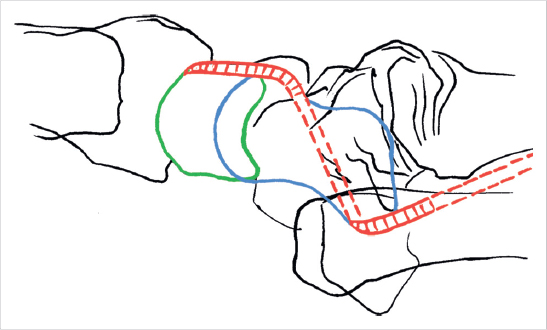
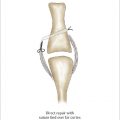
Brunelli initially described a technique to stabilize the unstable and flexed scaphoid in the setting of a scapholunate ligament (SLL) tear by passing half of a flexor carpi radialis (FCR) tendon—released proximally but anchored distally—through the axis of the scaphoid and securing it to the posterior distal radius to prevent scaphoid flexion and progression of scapholunate advanced collapse (SLAC) 1 (► Fig. 68.1). Several modifications of Brunelli’s reconstruction have been described subsequently to reconstruct the SLL in order to provide scaphoid stability while also preserving physiologic movement of the scaphoid (► Fig. 68.2).
68.2 Key Principles
There are several strategies for restoring scapholunate (SL) instability due to SLL disruption. A tendon slip of the FCR is utilized as a tendon graft. The graft stabilizes the scaphoid from distal (volar) to proximal (dorsal). Rotatory stability is achieved by securing the graft to either the dorsal distal radius (the original Brunelli technique), lunate bone, or other carpal structures (various modified Brunelli techniques).
68.3 Expectations
Patients may avoid progression to a SLAC wrist if scapholunate instability is addressed in a timely manner. 2 , 3 This technique restores anatomy and stability by reconstructing the SLL in an anatomic manner, while maintaining wrist range of motion which may be diminished with other reconstructive procedures such as a capsulodesis.
68.4 Indications
Patients are indicated for a Brunelli-type reconstruction if there is acute SL instability or subacute but reducible SL instability without development of SLAC changes. SL insufficiency or diastasis can be diagnosed by increased space between the scaphoid and lunate (► Fig. 68.3), flexed scaphoid, or extended lunate on lateral radiographs. 4

68.5 Contraindications
Chronic and/or unreducible scapholunate diastasis.
SLAC arthritic changes of the wrist.
Inflammatory arthritis of the wrist.
Related posts:
 62 Finger (PIP/DIP) Collateral Ligament Repair
62 Finger (PIP/DIP) Collateral Ligament Repair
 65 Thumb Metacarpophalangeal Joint Collateral Ligament Reconstruction
65 Thumb Metacarpophalangeal Joint Collateral Ligament Reconstruction
 66 Scapholunate Ligament Repair
66 Scapholunate Ligament Repair
 63 Finger Metacarpophalangeal Joint Collateral Ligament Repair
63 Finger Metacarpophalangeal Joint Collateral Ligament Repair
 67 Scapholunate Capsulodesis
67 Scapholunate Capsulodesis
 64 Thumb Metacarpophalangeal Joint Collateral Ligament Repair
64 Thumb Metacarpophalangeal Joint Collateral Ligament Repair
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


