64 Thumb Metacarpophalangeal Joint Collateral Ligament Repair
Abstract
Thumb metacarpophalangeal joint (MCPJ) collateral ligament repair is a treatment option in acute complete ligament tears and those associated with Stener lesions or MCPJ subluxation. Ulnar collateral ligament tears are more common than radial collateral ligament tears. While physical examination is typically sufficient for the diagnosis of complete tears, advanced imaging can be useful to fully delineate collateral ligament injuries in cases of clinical uncertainty. Repair of the collateral ligaments of the thumb can be performed with suture anchors. The key to the procedure is precise reattachment to the bony footprint.
64.1 Description
Treatment of thumb metacarpophalangeal joint (MCPJ) ulnar collateral ligament (UCL) injuries depends on acuity of the injury, location, partial versus complete rupture, and the presence of a Stener lesion. Acute (< 4 weeks old) injuries are often referred to as a Skier’s thumb and are amenable to primary repair, whereas chronic injuries are referred to as Gamekeeper’s thumb and frequently require ligament reconstruction. 1 , 2
Radial collateral ligament (RCL) injuries are far less common. Although a Stener type lesion (abductor aponeurosis rather than the adductor) can occur, it occurs less frequently with RCL tears. Physical examination may show a prominent dorsal prominence of the metacarpal head because of the rotational deformity caused by a torn RCL. Phalangeal subluxation may also suggest dorsal capsule injury in addition to a RCL tear. 1 , 2
64.1.1 Anatomy/Physiology
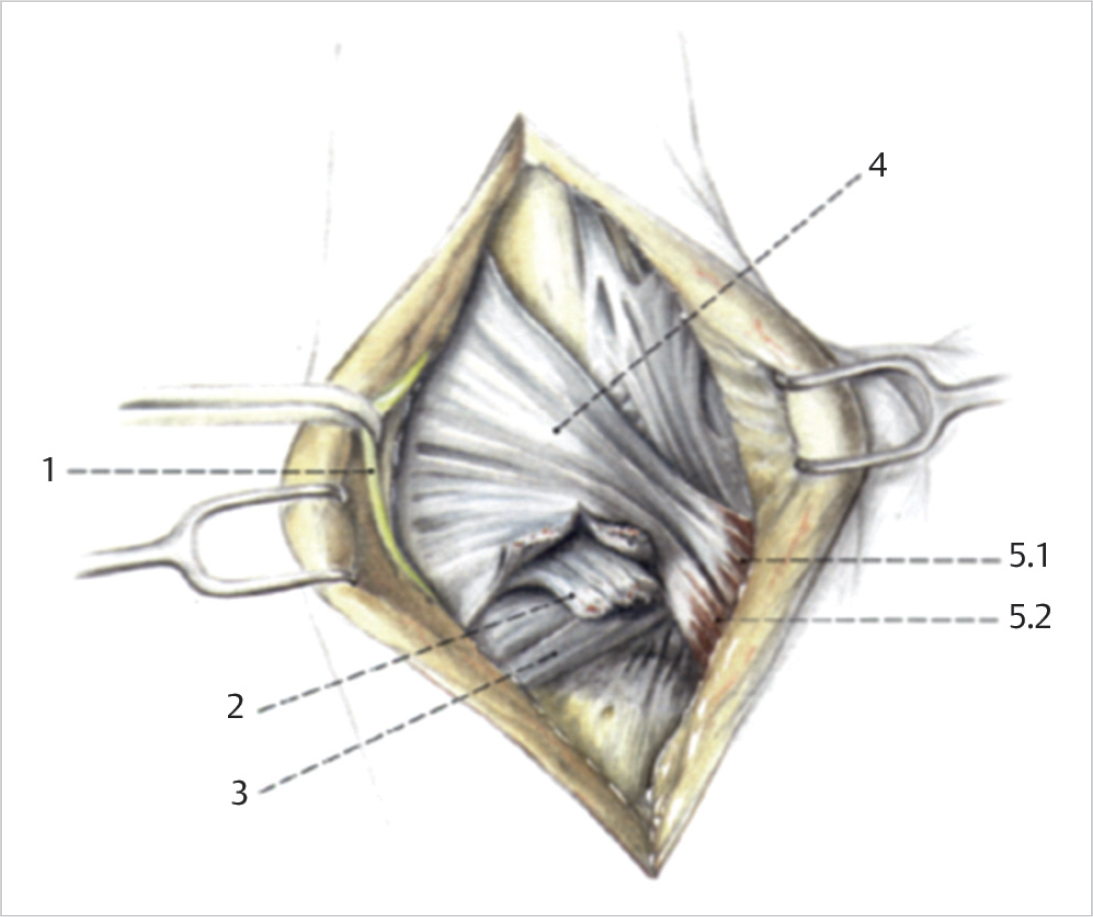
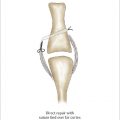
Thumb MPCJs, RCLs, and UCLs consist of both the proper ligament and the accessory ligament (► Fig. 64.1). The proper collateral ligament is mechanically important and functions as primary stabilizer of the MCPJ, originating from the lateral aspect of the metacarpal and inserting on the palmar portion of the lateral surface of the base of the proximal phalanx. It is lax in extension and taut in flexion due to the cam shape of the metacarpal head. The accessory collateral ligament originates from the metacarpal head and attaches on the volar plate. A Stener lesion occurs when the avulsed ligament becomes caught on the proximal edge of the adductor aponeurosis, precluding healing as the ligament stump is removed from its point of insertion (► Fig. 64.2).

64.2 Key Principles
Specific treatment of acute thumb UCL tears depends on location. Midsubstance tears are treated with direct suture repair, whereas distal avulsions are treated with suture anchor fixation back to bone. 1 , 2 The most important element of repair for both UCL and RCL tears is the precise anatomic realignment of the ligament to its bony footprint.
64.3 Expectations
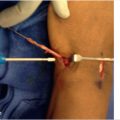
Following surgery, the thumb is immobilized with the interphalangeal joint left free for 3 to 4 weeks. Hand therapy is begun 3 to 4 weeks postoperatively and the patient is switched to a hand-based thermoplastic splint which should be worn an additional 2 to 4 weeks after removal of the postoperative splint or cast (► Fig. 64.3). Stiffness should be expected for several weeks to months following surgery. Unrestricted activity may be restarted approximately 3 to 4 months after surgery; some minor discomfort may continue up to 1 year following surgery. 2

64.4 Indications
Partial UCL ruptures can be treated nonoperatively within 3 to 4 weeks of continuous immobilization. Operative fixation is performed when any of the following criteria are met, although it is recommended that several tests be performed and considered together.
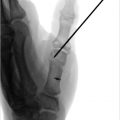
Greater than 30 degrees of laxity with radial stress (► Fig. 64.4).
Greater than 15 degrees of laxity with radial stress compared to the contralateral thumb.
Lack of a solid end point when stressing the MCPJ at 30 degrees of flexion. 3
Displacement of the UCL greater than or equal to 3 mm visualized on MRI. 4
Interposition of the adductor aponeurosis (Stener lesion), which can be found on MRI or ultrasound. This can occasionally be palpated on physical examination. 5 , 6
Complete RCL tear where progressive volar and ulnar subluxation of the MCPJ can occur due to the unopposed pull of the adductor aponeurosis.

Partial RCL tears can be treated like partial UCL tears. Complete RCL tears are diagnosed similar to tears of the UCL, although a Stener equivalent is usually not observed. A unique finding to RCL tears is volar subluxation on standard radiographs, which occurs more commonly than with complete UCL tears. Complete, acute tears should be treated with early surgical repair. 2 , 7 , 8
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


