66 Scapholunate Ligament Repair
Abstract
Complete rupture of the scapholunate (SL) ligament causes diastasis between the scaphoid and lunate, and subsequent instability that can lead to arthritic changes (scapholunate advanced collapse [SLAC] wrist). Surgical repair is warranted in acute ruptures and should be performed expeditiously. Various nuances with respect to the surgical procedure are described, but most importantly, an anatomic reduction of the SL interval is necessary. Suture anchors are used to repair the ligament, and often, a capsulodesis procedure will be performed to augment the repair. The SL interval is pinned in place with Kirschner (K) wires to maintain reduction while the soft tissue structures heal. The wrist is immobilized for 6 to 10 weeks postoperatively, at which point the pins are removed and the patient starts guided hand therapy. Diminished wrist motion, and subsequent widening of the scapholunate articulation is often observed during long term follow-up.
66.1 Description and Diagnosis
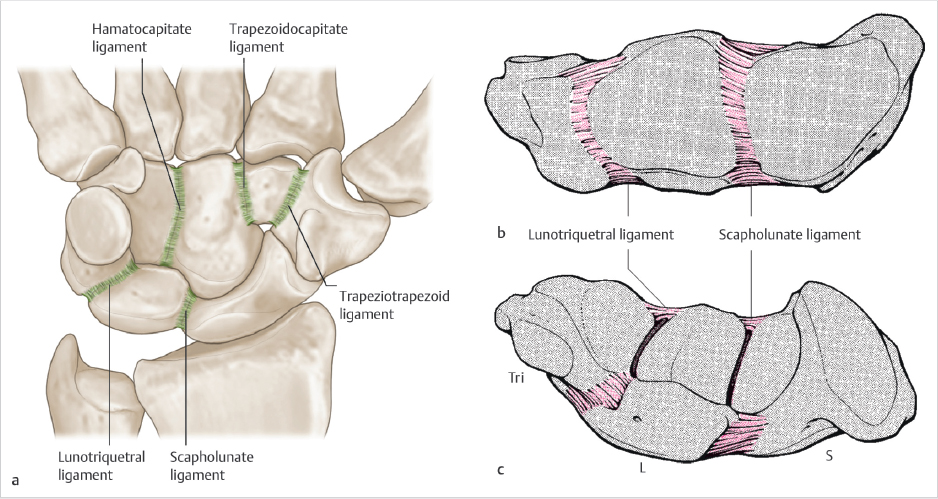
The scapholunate (SL) ligament is one of the mechanical cornerstones of the wrist joint (► Fig. 66.1) A rupture of this ligament has deleterious effects on wrist biomechanics, which can eventually lead to arthrosis. Pain after trauma located at the SL interval, often times associated with swelling, may represent a SL ligament tear. 1 There are many clinical and radiographic signs which may help to make the diagnosis. On physical examination, pain over the SL ligament and the presence of a positive Watson’s scaphoid shift test 2 may be indicative of a scapholunate interosseous ligament (SLIL) rupture.
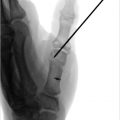
There are many radiographic indicators, including diastasis between the scaphoid and lunate on the PA radiograph greater than 3 mm (► Fig. 66.2a). Moreover, a clenched fist/pencil grip view (► Fig. 66.2b) drives open the SL interval and can accentuate the deformity. A cortical ring sign (► Fig. 66.2c) and an increased scapholunate angle (► Fig. 66.2d) are other indicators of this pathology. MRI studies are often performed (► Fig. 66.3), but have variable rates of sensitivity and specificity. 3 The gold standard for diagnosis of a SL ligament rupture remains diagnostic arthroscopy. The Geissler classification is used to characterize a tear. 4


66.2 Indications
Direct surgical repair is indicated for patients with acute wrist pain and a diagnosis of an acute SL ligament tear (< 6 weeks). Treatment for chronic injuries (> 6 weeks) is controversial, and options include direct repair with capsulodesis, tendon reconstruction, open reduction with screw fixation, and other techniques.
Related posts:
 65 Thumb Metacarpophalangeal Joint Collateral Ligament Reconstruction
65 Thumb Metacarpophalangeal Joint Collateral Ligament Reconstruction
 63 Finger Metacarpophalangeal Joint Collateral Ligament Repair
63 Finger Metacarpophalangeal Joint Collateral Ligament Repair
 69 Distal Radioulnar Ligament Repair/Reconstruction
69 Distal Radioulnar Ligament Repair/Reconstruction
 68 Scapholunate Ligament Reconstruction (Brunelli Types)
68 Scapholunate Ligament Reconstruction (Brunelli Types)
 67 Scapholunate Capsulodesis
67 Scapholunate Capsulodesis
 64 Thumb Metacarpophalangeal Joint Collateral Ligament Repair
64 Thumb Metacarpophalangeal Joint Collateral Ligament Repair
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


