63 Finger Metacarpophalangeal Joint Collateral Ligament Repair
Abstract
Injuries to the collateral ligaments of the fingers are less common than those sustained in the thumb. This injury can be functionally disabling if not properly diagnosed and treated appropriately. X-rays can be helpful in the workup of this injury and MRI can be a valuable diagnostic tool as well. Partial (Grade 1 and 2) injuries and nondisplaced fractures are treated conservatively. Complete (Grade 3) injuries and displaced fractures are treated surgically. For chronic injuries, direct repair is recommended if satisfactory ligament quality is present. When lig-ament quality is not satisfactory, tendon graft reconstruction is preferred. Clinical results of acute repair are usually better than chronic repair or reconstruction which emphasizes the importance of early diagnosis and treatment.
63.1 Description
Injuries to the collateral ligaments of the metacarpophalangeal (MP) joints of the index, long, ring, and small digits are less common than sustained in the thumb.
1 in 1,000 hand injuries are injuries to collateral ligaments, with 39% involving the fingers and 61% involving the thumb. 1
These injuries can be functionally disabling and are frequently neglected by the patient or underdiagnosed.
63.2 Anatomy/Physiology
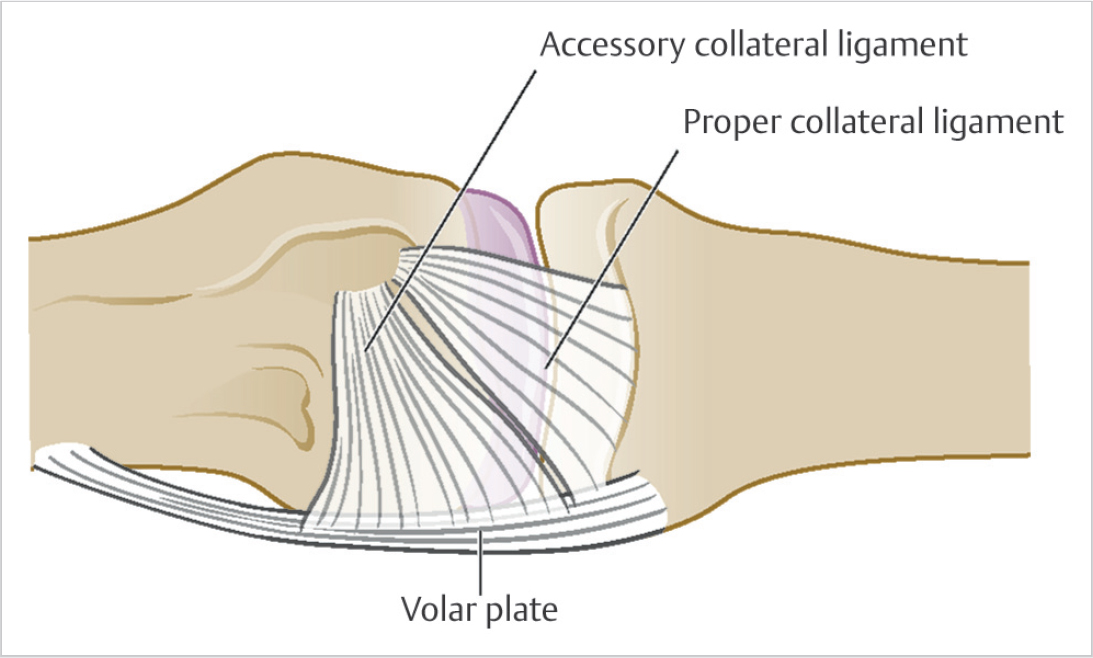
Finger MP joint radial and ulnar collateral ligaments consist of both the proper ligament and the accessory ligament (► Fig. 63.1).
The proper collateral ligament is the most important and strongest stabilizer of the MP joint, but in severe injuries, the accessory collateral ligament can be torn as well.
The proper collateral ligament is a thick cord which originates from the posterior tubercle on the lateral surface of the metacarpal head, which is in a slightly dorsal position, and courses obliquely to insert on the palmar portion of the lateral surface of the base of the proximal phalanx.
The proper collateral ligaments are the main static restraints, with the MP joints in maximum flexion.
The accessory collateral ligament is a fan-shaped structure that originates from the apex of the anterior tubercles of the lateral surface of the metacarpal head and spreads toward the palm to insert along the lateral margin of the volar plate.
The accessory collateral ligaments along with the volar plate are the main static restraints with the MP joints in full extension.
Fingers MP joints are most lax in extension and become progressively tighter with flexion, mainly due to the cam shape of the metacarpal head causing an overall lengthening and therefore tightening of the proper collateral ligament with increasing joint flexion. 2
63.3 Examination
Stability of the collateral ligament is best assessed with the MP joint in full flexion.
Baseline examination of the opposite side noninjured similar digit is very important in providing a normal for comparison. 3
63.4 Clinical Aspects
Injuries to the finger collateral ligaments are most common in the 4th decade and occur slightly more commonly in men than women.
This injury occurs due to an abduction or adduction force with the MP joint in some degree of flexion.
The middle finger is most commonly injured with both radial and ulnar collateral ligaments equally affected.
The radial collateral ligament is more commonly injured than the ulnar collateral ligament in the ring and small digits.
The ulnar collateral ligament is more commonly injured in the index finger, although injury of the radial collateral ligament of the index finger may be a very functionally disabling injury due to the importance of this ligament with thumb to index pinch.
Collateral ligaments may be avulsed from bone with either a large or small attached fracture fragment.
63.5 Ligament Injury Grades/Classification
63.5.1 Grade 1
Ligament becomes stretched with a few torn fibers.
No laxity is present on physical examination.
63.5.2 Grade 2
There is a greater number of torn ligament fibers.
More pain and swelling noted clinically.
Increased laxity on clinical examination with a definite endpoint.
63.5.3 Grade 3
All ligament fibers are torn.
Marked laxity on exam with no definite endpoint
63.5.4 Fractures
Small avulsion fragment.
Larger bone fragment.
63.6 Location of Ligament Injury
Avulsion from the proximal phalanx (most common).
Midsubstance ligament tear.
Avulsed from the metacarpal (least common).
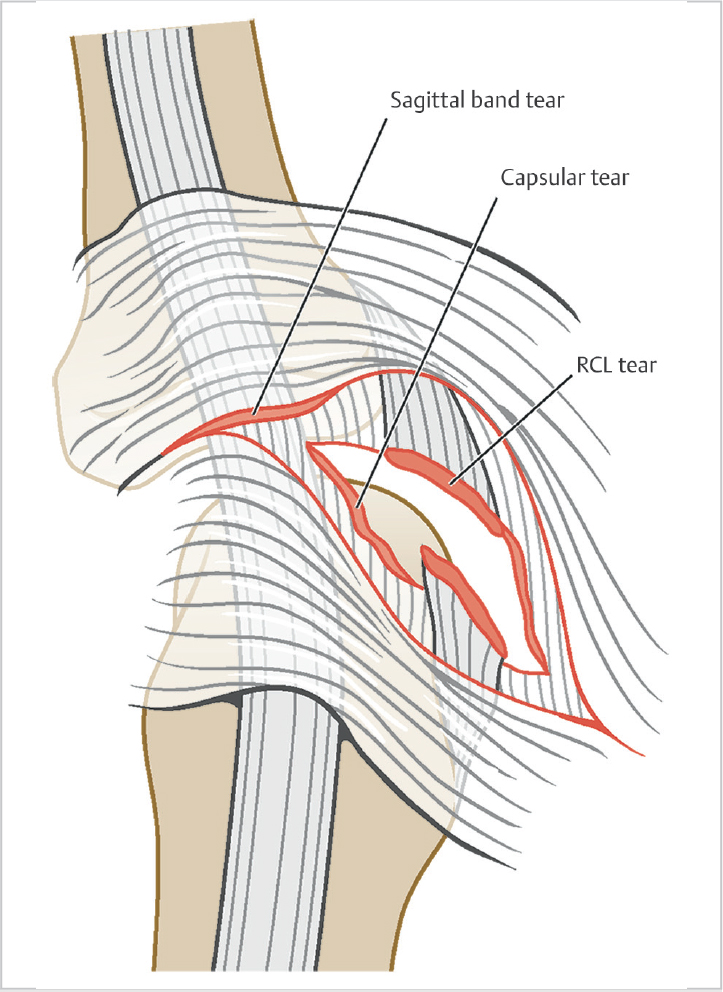
Disruption of the sagittal band may also be seen in these injuries and can become entrapped at the site of the ligament tear, which is similar to a Stener’s lesion of the thumb 4 (► Fig. 63.2).
Related posts:
 65 Thumb Metacarpophalangeal Joint Collateral Ligament Reconstruction
65 Thumb Metacarpophalangeal Joint Collateral Ligament Reconstruction
 66 Scapholunate Ligament Repair
66 Scapholunate Ligament Repair
 69 Distal Radioulnar Ligament Repair/Reconstruction
69 Distal Radioulnar Ligament Repair/Reconstruction
 68 Scapholunate Ligament Reconstruction (Brunelli Types)
68 Scapholunate Ligament Reconstruction (Brunelli Types)
 67 Scapholunate Capsulodesis
67 Scapholunate Capsulodesis
 64 Thumb Metacarpophalangeal Joint Collateral Ligament Repair
64 Thumb Metacarpophalangeal Joint Collateral Ligament Repair
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


