Pinta
The histopathological changes in pinta are largely similar to those in yaws [49,50,52], except that ulcer formation does not occur [49]. In the early lesion, only mild acanthosis is present, with migration of some lymphoid cells into the epidermis. Basal cells show loss of melanin and liquefaction degeneration. In early-stage lesions, melanophages may be seen in the upper dermis [50]. A moderate dermal inflammatory infiltrate consists mainly of plasma cells and lymphocytes. Histiocytes and neutrophils may be seen. Occasionally, slight swelling of endothelial cells is present [49,50]. In the late stage, irregular acanthosis or epidermal atrophy can occur. Pigmentary changes vary with the colour of skin lesions. A lymphocytic infiltrate and numerous melanophages may be present in the dermis. Treponemes can sometimes be visualized in the epidermis by means of silver staining methods or immunofluorescent techniques. Dyschromic late skin lesions may contain treponemes and show an inflammatory infiltrate, but achromic late skin lesions lack both of these features [50].
Endemic Syphilis
The histopathological picture closely resembles that of venereal syphilis. In the early stage, the dermal infiltrate is primarily perivascular, and plasma cells and lymphocytes predominate. Slight vascular changes may be present. In early endemic syphilis, granulomas consisting of epithelioid cells and multinuclear giant cells are seen [50]. Silver or immunofluorescent staining methods may assist in visualization of the treponemes in the early stage. In the late stage, treponemes are rarely seen.
Clinical Features
Yaws
Historically, several systems have been used to classify the clinical stages of yaws [6]. The most frequently used system defines four stages (primary, secondary, tertiary and latent), equivalent to those seen in venereal syphilis. In the primary stage, skin lesions develop at the site of infection. Secondary stage skin lesions, a result of the widespread dissemination of treponemes, resemble the initial skin lesions, but are greater in both number and size. In the tertiary stage, deformities can occur. An overlap between the stages is often noted. A more practical system of classification defines an early stage with contagious skin lesions, and a late stage, in which the skin lesions are less contagious [44]. Early yaws includes the primary and secondary stage; late yaws is equivalent to the tertiary stage.
Early stage skin lesions, often pruritic, appear after an incubation period of 9–90 days, with an average of 3 weeks [6]. Classically, the initial presentation of yaws consists of one or more non-tender papules, which later become crusted and ulcerated (Fig. 60.3). The lower extremities are a site of predilection. The early papules can evolve into ulcerated and papillomatous lesions, containing numerous treponemes.

Disseminated lesions may occur together with or after the disappearance of primary lesions. These are sometimes preceded or accompanied by malaise, fever and generalized lymphadenopathy. These early (secondary) stage skin lesions often resemble the initial lesions (Fig. 60.4). Macules, papules and nodules can occur. Palms and soles often show hyperkeratosis (crab yaws). In the early stage, bone and joint manifestations, particularly osteitis and periostitis, may already be noted [53]. Lesions in the early stage of yaws usually disappear spontaneously, sometimes leaving slight pigmentary changes. However, severe secondary infection can be life-threatening and scarring is common. In the warm and rainy seasons, cutaneous lesions are more florid and abundant than during drier periods of the year. During the dry season, patients may present with atypical macular cutaneous lesions.
Fig. 60.4 Multiple ulcerocrustopapillomatous skin lesions in early (secondary) yaws. Dark-field examination revealed the presence of many treponemes.

After the early skin manifestations have subsided, a latent period of variable duration follows. The presence of latent infection can be detected by the presence of a positive serological test. This period may be interrupted by one or more relapses of skin lesions. In the majority of patients latency is lifelong. However, an estimated 10% of patients develop a destructive late stage after 5–10 years or longer. Irreversible lesions of bone, cartilage, soft tissue and the skin then develop. Manifestations of late yaws include gangosa (destructive ulcerative rhinopharyngitis), gummata, juxta-articular nodes, contractures and sabre tibiae (Figs 60.5 and 60.6). Gondou, the rarely occurring exostoses of nasal and adjacent bones, can also develop early in the course of the disease. Hyperkeratotic lesions may be observed in both late and early yaws [6].
Fig. 60.5 Sabre tibia. This irreversible condition is caused by chronic untreated periostitis.
Reproduced from Perine et al. 1984 [6] with permission.

Fig. 60.6 Gummatous osteoperiostitis. Monodactylitis is characteristic of late yaws bone lesions. Deformity of the fingers may result.
Reproduced from Perine et al. 1984 [6] with permission.

It has been generally assumed that no neurological or cardiovascular involvement occurs in yaws. However, a review in 1986 suggests that cardiovascular and neurological disease, similar to that in syphilis, may be seen in patients with yaws [54]. In one study, ocular and neurological abnormalities were described in patients with late yaws [55]. Cerebrospinal fluid abnormalities, optic atrophy, abnormal pupils and perivascular sheathing were noted. As confusion between yaws and other treponematoses is possible, and as there is no serological test to differentiate between these diseases, additional research is required [54].
Pinta
The early stage of pinta includes the development of initial lesions and more generalized secondary lesions; the late stage includes a tertiary and late latent phase. There may be considerable overlap between stages. After an incubation period of several weeks to months, the initial lesion, usually a papule or an erythematosquamous plaque, develops on exposed skin. This primary lesion may become pigmented, hyperkeratotic and scaly, and may be accompanied by local lymphadenopathy. Primary lesions of pinta disappear spontaneously.
After several months or even years, more extensive and generally smaller lesions may appear, which are similar in morphology to the initial lesions. These so-called ‘pintids’ may persist for years or resolve and then recur. Striking changes in skin pigmentation may result [6].
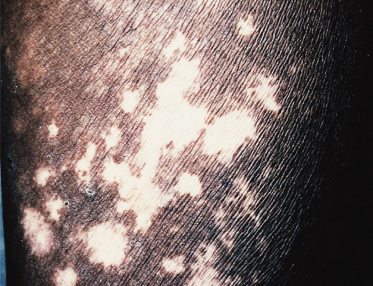
In late (tertiary) pinta, disfiguring pigmentary changes, achromia, skin atrophy and hyperkeratoses are common. The pigmentary alteration may vary from lesion to lesion, resulting in a sometimes lifelong mottling of the skin (Fig. 60.7). Skin lesions may turn red, white, bluish, violet or brown. Severe mutilation does not occur; it is assumed that the skin is the only organ affected by this chronic treponemal disease [6]. Pinta is considered the most benign of the endemic treponematoses, with a good prognosis. No cardiological or neurological symptoms have been described [6,7,55]. There is no known congenital form [7].
Endemic Syphilis
Endemic syphilis may be divided into an early and a late stage. The early stage includes primary and secondary symptoms, and the late stage includes tertiary and late latent disease. In contrast with the other treponematoses, and perhaps because of the small inoculum, primary lesions may go unrecognized. In the primary phase, the oropharyngeal mucosa is frequently involved. Frequently, endemic syphilis first manifests in the secondary stage and resembles secondary venereal syphilis. Patches on the mucous membranes, angular stomatitis, non-pruritic skin eruptions and generalized lymphadenopathy are the most common manifestations. Condylomata lata, comparable to those in yaws and sexually transmitted syphilis, occur frequently. In the early stage, a painful osteoperiostitis, similar to yaws, may be observed. After early lesions have subsided, the patient enters latency. In this stage, treponemal infection can only be detected by positive serological tests. In some patients, the late stage may develop at a young age [36,42]. In this stage, affection of skin, bones and cartilage may lead to severe destruction, especially of the nose and palate. The larynx may be solely affected [43]. In patients with nasopharyngeal involvement, gummata may progress to destructive chronic ulceration, similar to rhinopharyngitis mutilans. Neurological and cardiological involvement is extremely rare or perhaps non-existent [42,43,56,57].
Differential Diagnosis.
The diagnosis of endemic treponematosis must be based on clinical, geographical, epidemiological and laboratory findings. At this point in time, it is not possible to distinguish between the causative agents of the different treponemal diseases on serological, morphological or biochemical grounds. Positive serological tests in all but the very early stage, the presence of treponemes in dark-field examination of exudates of cutaneous lesions and the histopathological features confirm the diagnosis. Diagnosis can be difficult in geographical regions where venereal syphilis and/or endemic treponematoses are simultaneously prevalent, particularly for patients who are in latency and the late stage (Table 60.2). Several other diseases in the tropics can resemble yaws, pinta and endemic syphilis (Tables 60.3–60.5).
Table 60.2 Some characteristics of treponematoses
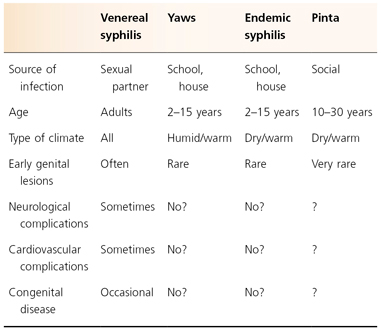
Table 60.3 Differential diagnosis of yaws
| Skin lesions |
| Venereal syphilis |
| Endemic syphilis |
| Pinta |
| Leprosy |
| Impetigo |
| Ecthyma |
| Tungiasis |
| Tropical ulcers |
| Chromomycosis |
| Cutaneous leishmaniasis |
| Sarcoidosis, psoriasis |
| Vitamin deficiencies |
| Scabies |
| Viral infections such as mollusca contagiosa or plantar warts |
| Bone lesions |
| Venereal syphilis |
| Endemic syphilis |
| Tuberculosis |
| Bacterial osteomyelitis |









