Abstract
This chapter will provide the reader a concise overview of various traumatic injuries that are commonly encountered in the hand. The osseous structures of interest described in this section include the metacarpals and phalanges. For each pathology summarized, emphasis is placed on descriptions of the mechanism of injury, relevant anatomy, clinical presentation, appropriate imaging, and recommended treatments. Figures with radiographs are also provided to illustrate key pathologies and treatments. This chapter is designed to provide an easily readable reference that will aid the orthopaedic practitioner in determining appropriate treatment for a traumatic pathology encountered during consultations in the emergency department, inpatient ward, or outpatient clinic. Thus, it will ideally be a useful resource for orthopaedic residents, advanced practitioners, and practicing orthopedic surgeons. References for the core material outlined here are listed at the end of this chapter and contain further information on each topic presented for the interested reader.
6 Fractures, Dislocations, and Ligament Injuries of the Hand
I. Fractures of the Metacarpals
A. Thumb Metacarpal Base Fractures
Mechanism of injury
Relevant anatomy and epidemiology
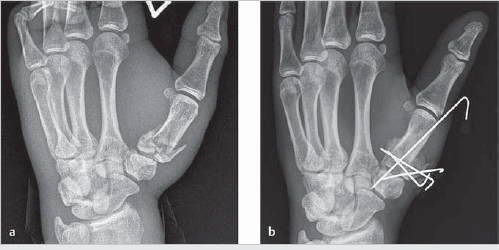
Fractures can be extra-articular, intra-articular with a stable volar-ulnar fragment (a Bennett’s fracture), or intra-articular with comminution (a Rolando’s fracture, see ► Fig. 6.1a).
Deforming forces: Adductor pollicis, abductor pollicis longus, and extensor pollicis longus.
Clinical presentation
Pain, swelling, and limited range of motion (ROM) at the base of the thumb.
Imaging used for diagnosis
Thumb X-ray series is best for diagnosis and to evaluate for intra-articular extension.
Treatment
Nonoperative: Stable, extra-articular, and <30 degrees of angular deformity can be splinted.
Operative: If unstable or intra-articular, then proceed with open reduction internal fixation (ORIF) versus closed reduction percutaneous pinning (CRPP) (► Fig. 6.1b).
B. Metacarpal Base Fractures Other than the Thumb
Mechanism of injury
Direct trauma (e.g., from punch) is the mechanism ofall non-thumb metacarpal fractures. 1 , 2 , 3 , 4
Relevant anatomy and epidemiology
May be extra-articular or intra-articular, usually apex dorsal due to intrinsic forces.
It is important to evaluate for concomitant carpometacarpal (CMC) joint dislocation.
Clinical presentation
Pain and swelling in middle hand present, sometimes with open wounds or tenting of skin.
Evaluate all metacarpal fractures for malrotation by confirming that the cascade of fingertips, when the patient makes a closed fist, points to the scaphoid.
Imaging used for diagnosis
Usually, a full hand X-ray series suffices to diagnose all metacarpal fractures.
Treatment
Nonoperative: Treat with reduction and splinting in intrinsic plus position for:
A nondisplaced intra-articular fracture.
An extra-articular fracture with no malrotation and with acceptable angulation (10 degrees for index [IF], 20 degrees for long [LF], 30 degrees for ring [RF], and 40 degrees for small [SF] fingers).
Operative: If none of the above, consider proceeding to ORIF with plate versus CRPP.
C. Metacarpal Shaft Fractures
Relevant anatomy and epidemiology
Fractures may have transverse or oblique orientation, with the latter prone to shortening. 1 , 2 , 3 , 4
Treatment
Nonoperative: Can do closed reduction and immobilization if no malrotation and acceptable angulation (10 degrees for IF, 20 degrees for LF, 30 degrees for RF, and 40 degrees for SF).
Operative: Consider ORIF with plate/screws versus CRPP for oblique fractures (► Fig. 6.2).

D. Metacarpal Head and Neck Fractures
Relevant anatomy and epidemiology
Treatment
Nonoperative: Can be treated with reduction and splinting in intrinsic plus position for nondisplaced intra-articular head or extra-articular neck fractures (with no malrotation and acceptable angulation of 10-15 degrees for IF and LF, up to 40 degrees for RF, and up to 60 degrees for SF).
Operative: If none of the above, consider ORIF with plate/screws versus CRPP versus head arthroplasty (if a high degree of comminution is present).
Related posts:
 8 Fractures and Dislocations of the Distal Radius and Ulna
8 Fractures and Dislocations of the Distal Radius and Ulna
 3 Radiographic Anatomy
3 Radiographic Anatomy
 12 Tendinitis, Tendinosis, and Dupuytren’s Contracture
12 Tendinitis, Tendinosis, and Dupuytren’s Contracture
 15 Extensor Tendon Injury, Repair, and Reconstruction
15 Extensor Tendon Injury, Repair, and Reconstruction
 Private: 20 Vascular Pathology of the Hand and Upper Extremities, including Kienbock’s Disease
Private: 20 Vascular Pathology of the Hand and Upper Extremities, including Kienbock’s Disease
 Private: 25 Fractures of the Pediatric Hand
Private: 25 Fractures of the Pediatric Hand
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


