Abstract
Extensor tendons are susceptible to injury because of their superficial location. Along with ligamentous structures and intrinsic musculature, they provide stability to the different articulations of the hand and allow for range of motion. Extensor tendon injuries are classified based their location (Zones I-VIII), with each zone having its own characteristic presentations and management. Diagnosis is usually clinical, with various imaging modalities available as adjuncts. Treatment may be nonoperative or surgical, depending on injury zone and chronicity. Primary repair is performed when the gap needed to bridge is small. Certain suture techniques have been shown to be superior in each injury zone, taking into consideration the increasing thickness of the extensor tendons as the injury becomes more proximal. Reconstruction techniques are varied, depending on injury zone and surgeon’s preference and can be used in cases where pri-mary repair is not feasible. Postinjury rehabilitation options include early active mobilization and dynamic splinting regimens, which are important to avoid complications such as adhesions, loss of range of motion, and tendon shortening.
15 Extensor Tendon Injury, Repair, and Reconstruction
I. Introduction
II. Anatomy
A. Extrinsic Extensor Muscles
Originate in the elbow and forearm.
Superficial group: Extensor carpi radialis longus (ECRL), extensor carpi radialis brevis (ECRB), extensor digitorum communis (EDC), extensor digiti minimi (EDM), and extensor carpi ulnaris (ECU).
Deep group: Abductor pollicis longus (APL), extensor pollicis brevis (EPB), extensor pollicis longus (EPL), and extensor indicis proprius (EIP).
ECRL is innervated by the radial nerve, ECRB innervated by the posterior interosseous nerve (PIN) or superficial radial sensory nerve, 3 , 4 and the remaining muscles by the PIN.
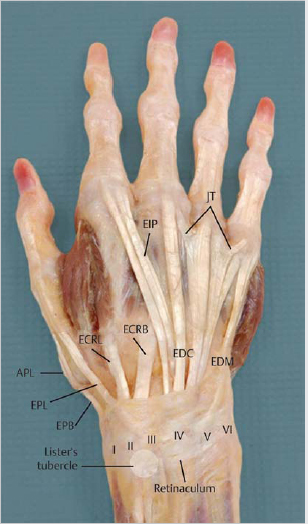
Extrinsic extensor muscle tendons travel through six compartments in the dorsal aspect of the wrist, covered by the extensor retinaculum (► Fig. 15.1).
First compartment: APL and EPB tendons.
Second compartment: ECRL and ECRB tendons, with ECRB located ulnar to ECRL.
Third compartment: EPL.
Fourth compartment: Four tendons of EDC and EIP tendon.
EIP is commonly located ulnar to the index finger EDC.
Contains terminal branch of PIN, which provides sensory and proprioceptive fibers to dorsal wrist capsule.
Fifth compartment: EDM.
Sixth compartment: ECU.
B. Intrinsic Muscles
Originate and insert within the hand.
Four lumbrical muscles, numbered sequentially from radial to ulnar:
Originate from flexor digitorum profundus tendons.
Insert onto the lateral band on the radial side ofeach proximal phalanx.
First and second lumbricals are innervated by the median nerve, third and fourth lumbricals are innervated by the ulnar nerve.
Function is to flex metacarpophalangeal (MCP) joints and extend interphalangeal (IP) joints.
Seven interossei muscles: Three palmar interossei and four dorsal interossei:
Originate from the metacarpals.
Insert onto the proximal phalanges and extensor expansions.
Innervated by the ulnar nerve.
Function is to abduct and adduct the fingers.
C. Tendons
Extrinsic tendons run over MCP joints, then trifurcate into a central slip and two lateral slips:
The central slip inserts at the base of the middle phalanx.
The lateral slips insert at the base of the distal phalanx as a single terminal extensor tendon.
Intrinsic tendons form lateral bands on each side of the digits, which join the extensor mechanism just proximal to the proximal interphalangeal (PIP) joints (► Fig. 15.2).
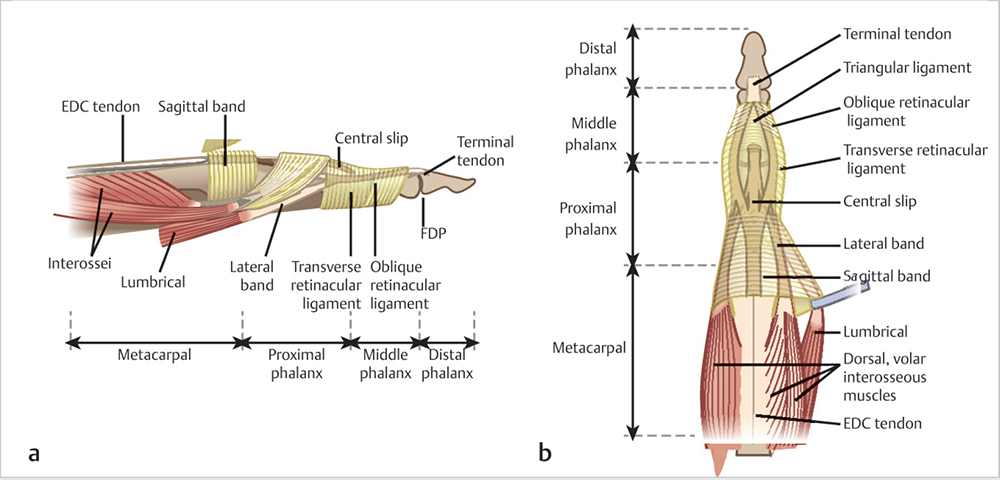
D. Additional Stabilizers
Juncturae tendinum: Interconnect EDC tendons proximal to the MCP joints.
Sagittal bands: Form a sling around the extensor tendons to maintain their central position, attaching them to the volar plate at the level of the MCP joints.
Transverse retinacular ligaments: Prevent dorsal subluxation of the conjoined lateral bands at the level of the PIP joint.
Disruption results in swan neck deformity: PIP hyperextension with distal interphalangeal (DIP) flexion.
Triangular ligament: Prevents volar subluxation of the conjoined lateral bands by connecting them at the level of the middle phalanx.
Disruption results in boutonniere deformity: PIP flexion and hyperextension of the DIP.
Oblique retinacular ligaments: Coordinate PIP and DIP joint movements. 5
III. Injury Zones
A. Location
Injury zones are based on location, as described by Kleinert and Verdan (► Fig. 15.3). 6
Zone I: DIP joint. Injuries are further categorized based on Doyle’s classification 7 :
Type 1: Closed, with or without avulsion fracture (most common pattern).
Type 2: Open injury.
Type 3: Open injury with loss of soft tissue coverage and tendon substance.
Type 4:
Type 4a: Transepiphyseal fracture in children.
Type 4b: Phalanx base fracture involving 20 to 50% of articular surface.
Type 4c: Phalanx base fracture involving 50% or more of articular surface.
Zone II: Middle phalanx.
Zone III: PIP joint.
Zone IV: Proximal phalanx.
Zone V: MCP joint.
Sagittal band injuries occur at this level and can be classified into three types 8 :
Type 1: Contusion with no tendon tear.
Type 2: Tendon subluxation.
Type 3: Dislocation of tendon between metacarpal heads.
Zone VI: Dorsal hand.
Zone VII: Dorsal retinaculum.
Tendon ruptures may also present in association with rheumatoid arthritis:
Vaughan-Jackson syndrome: Rupture of extensor tendons resulting from dorsal ulnar head prominence, affecting EDM tendon first and proceeding radially.
Caput ulna syndrome: Synovitis in distal radioulnar joint leads to capsular and ECU sheath stretching with ECU volar subluxation, eventually leading to a prominent ulna causing additional stress over the already weakened tendons.
Zone VIII: Distal third of the forearm.

Related posts:
 6 Fractures, Dislocations, and Ligament Injuries of the Hand
6 Fractures, Dislocations, and Ligament Injuries of the Hand
 8 Fractures and Dislocations of the Distal Radius and Ulna
8 Fractures and Dislocations of the Distal Radius and Ulna
 14 Flexor Tendon Injury, Repair, and Reconstruction
14 Flexor Tendon Injury, Repair, and Reconstruction
 12 Tendinitis, Tendinosis, and Dupuytren’s Contracture
12 Tendinitis, Tendinosis, and Dupuytren’s Contracture
 Private: 20 Vascular Pathology of the Hand and Upper Extremities, including Kienbock’s Disease
Private: 20 Vascular Pathology of the Hand and Upper Extremities, including Kienbock’s Disease
 Private: 25 Fractures of the Pediatric Hand
Private: 25 Fractures of the Pediatric Hand
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


