5 Abnormal Eyelashes
Abstract
“Abnormal Eyelashes” discusses the condition in which eyelashes contact and irritate the eyeball in the absence of eyelid entropion; this is called trichiasis if the eyelash grows in the normal position but gets turned toward the globe, or distichiasis if the eyelash grows from an abnormal position. If eyelashes abrade the cornea, the patient will experience constant irritation, photophobia, and lacrimation. Constant corneal abrasion by ingrowing eyelashes can result in severe visual morbidity (e.g., corneal scarring seen in advanced trachoma). Simply epilating the offending eyelash is not recommended because it will regrow and be short and stiff, causing more corneal damage than the mature eyelash did. Treatment by electrolysis, argon laser ablation, cryotherapy, or wedge excision and the attendant postoperative care are described in detail.
5.1 Introduction
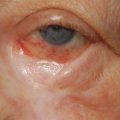
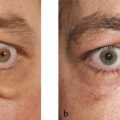
Trichiasis refers to a condition in which aberrant eyelashes turn inward against the globe in the absence of any eyelid malposition (Fig. 5‑1a). It is commonly associated with chronic blepharoconjunctivitis or cicatrizing conjunctivitis (e.g., ocular cicatricial pemphigoid). It may also be seen after eyelid margin trauma or after a poor surgical repair of the eyelid margin (e.g., after a wedge resection of an eyelid lesion). In contrast, distichiasis refers to a condition in which accessory eyelashes arise from the lid margin in an area other than the normal ciliary line, such as from the meibomian gland orifices (Fig. 5‑1b). If eyelashes abrade the cornea the patient will experience constant irritation, photophobia, and lacrimation. Fluorescein staining of the cornea will occur. Constant corneal abrasion by ingrowing eyelashes can result in severe visual morbidity (e.g., corneal scarring seen in advanced trachoma). Very rarely, abnormal eyelashes may be seen growing from an unusual location in the eyelid (Fig. 5‑1c).
The management of misdirected lashes because of an eyelid malposition is addressed in Chapters 3 and 4.

5.2 Management
Epilation
Bandage contact lens
Electrolysis
Argon laser ablation
Cryotherapy
Surgical excision
5.2.1 Epilation
Epilation of eyelashes provides a temporary relief from symptoms, but the symptoms are often exacerbated as the eyelashes regrow. The eyelashes are initially short and firm and create more corneal damage. Epilation also prevents definitive treatment by electrolysis. The surgeon is unable to identify the offending eyelashes until these have begun to regrow.
5.2.2 Bandage Contact Lens
A temporary relief from symptoms can be obtained by the fitting of a bandage contact lens while definitive treatment is being arranged. The contact lens has to be worn continuously, which exposes the patient to a risk of bacterial keratitis.
5.2.3 Electrolysis
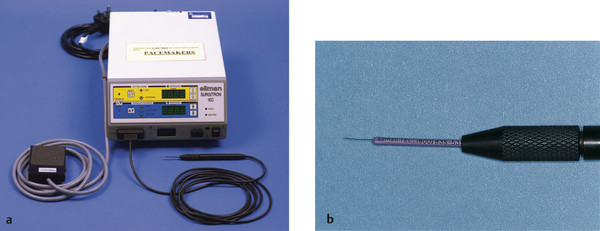
Electrolysis is an appropriate form of treatment if only a few eyelashes are present, particularly if they are located in different positions in the eyelids. The Ellman-Surgitron radiofrequency device is particularly suited for electrolysis if the patient does not have a cardiac pacemaker (Fig. 5‑2).
Surgical Procedure
A topical anesthetic agent is instilled into the eye.
Between 1 and 2 mL of 2% lidocaine with 1:80,000 units of adrenaline are injected subcutaneously and subconjunctivally into the affected eyelid.
The neutral plate is positioned between the patient’s shoulder blades.
The eyelid is grasped with a pair of Paufique forceps. The electrolysis needle is inserted along the lash to a depth of approximately 2 to 3 mm to the position of lash bulb using an operating microscope.
The current is applied for only 2 to 3 seconds using the foot pedal. The procedure is always initiated using the lowest settings on the device.
A gentle bubbling should be observed. The lash should either accompany the electrolysis needle as it is withdrawn or come out of the eyelid easily using epilation forceps but without any resistance. If there is any resistance, the procedure should be repeated.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


